International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 512
ISSN 2229-5518
Ultrasound Guided Fine Needle Aspiration Cytology with Evaluation of Pathological Distribution of Thyroid Nodules and Correlation with Post Operative Histopathology in Malignant Nodules
Laly Jose, Sara Ammu Chacko, Simi.
—————————— ——————————
Thyroid nodules are extremely common in the adult. In general almost 5% of the adult population has a palpable thyroid nodule. Sonographic screening of clinically normal thyroid glands can detect one or more thyroid nodules in about 50% of patients [1], [2], [3]. Although most thyroid nodules are benign, the possibility of malignancy needs to be excluded in thyroid nodules. Sonography is very sensitive to detect thyroid nodules. Its ability to differentiate benign and malignant nodule is relatively low [4]. In patients with thyroid nodules fine needle aspiration cytology has power to be an effective tool for diagnosis of malignancy.
————————————————
The purpose of the study is to evaluate the pathological distribution of thyroid nodules by ultrasound guided fine needle aspiration cytology and its correlation with post operative pathology in malignant nodules.
The study was conducted on 150 subjects referred from surgical OPD of Dr. SMCSI Medical College Hospital, Karakonam, Thiruvananthapuram for a period of 3 years.
Inclusion criteria were patients with 1. All nodules
> 8mm size. 2. Patients with single and multiple thyroid nodules.
Exclusion criteria included 1. Normal thyroid gland. 2. Diffusely enlarged thyroid without nodules.
3. Cases were no consent was obtained.
Ethical clearance was obtained from institutional review board for this study.The study was done using
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 513
ISSN 2229-5518
Siemens Sonoline -50 ultrasound scanner with colour and duplex Doppler.
US guided FNA technique. Pre procedural planning
Informed consent was obtained after discussing the purpose and procedure with the patients. A screening test for coagulation is not routinely need, but the patient was carefully questioned about recent or current anticoagulant therapy.
For US guided FNA the patient was placed in supine position with neck slightly extended. After the lesion is localised the overlying skin is cleansed with 10% povidone iodine solution and area was draped. A high resolution (7.5-15MHz) linear array transducer with sterile cover placed over its head was used. Ultrasound gel is not necessary because the povidone iodine solution used for skin sterilization also serves as primary coupling agent [5].
The collected material was placed on glass slide and smeared and fixed in 95% ethyl alcohol. The syringe was rinsed with normal saline solution to obtain any remaining material for use in cell blocking.
In 150 subjects studied, the incidence of malignancy as per histopathology report was 12% (n= 18).
A local anesthesia may be used approximately 1-
2ml of 1% lignocaine hydrochloride solution was injected to skin and superficial subcutaneous tissue at the predetermined site.
A 22-23G needle was used with attached 2-10ml syringe transducer is placed directly over the lesion. Before aspiration scanning was done in transverse plane for lesion localization followed by colour doppler mapping to depict any large blood vessels in and around the nodule. The
70
59.3
60
50
40
30 22
20
10
0
3.3 3.3 6.7 3.3 2
patient was instructed not to swallow or speak during insertion of needle. The needle tip was carefully monitored during procedure. At least 2 passes were done routinely.
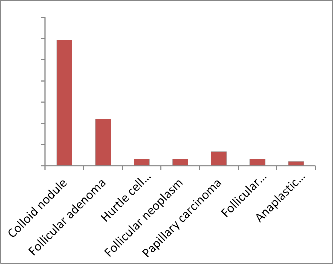
The commonest lesion was colloid nodules (n=89)
followed by follicular adenoma. The commonest malignant
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 514
ISSN 2229-5518


lesion was papillary carcinoma (n=10). In 5 cases FNAC showed follicular neoplasm and could not differentiate between follicular adenoma and follicular Ca. However surgery done in two cases out of the 5 cases reported as follicular neoplasm (by FNA) showed follicular adenoma on post operative histopathology.
Fig. 4 Well defined hypoechoic nodule with micro right lobe-Colloid nodule on FNAC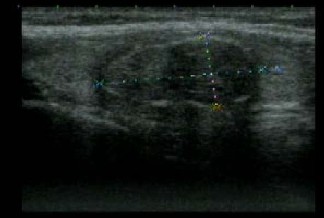

Fig. 2 Isoechoic nodule right lobe; Adenoma thyroid on FNAC
Fig. 3 Heterogenous nodule left lob; Colloid nodule on FNAC
Fig. 5. Well defined hypoechoic nodule calcification- Papillary Ca on FNAC
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 515
ISSN 2229-5518
The age of patients studied ranged from 9 to 65. Largest number of cases was in 3rd decade.
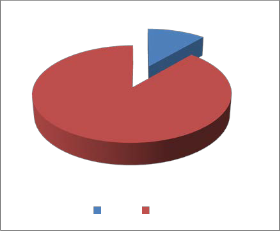
Sex | Number | Percentage |
Male | 17 | 11.3 |
Female | 133 | 88.7 |
FNAC and post operative pathology correlation was 100% for papillary and anaplastic carcinoma. In case of f 5 follicular carcinoma diagnosed by FNAC, one turned
out to be follicular adenoma.
88.7
11.3
Male Female
30
25
20
15 11.7
10
5
0
19.3
27.3
24
16.7
0.2
The commonest pathological entity encountered
was colloid nodule (n=89). Among benign lesions colloid nodule was the most common. Among malignant neoplasm, papillary carcinoma was the most common. The maximum number of cases occurred in 31-39 age group. In this age group the maximum number of benign lesion was colloid nodule. In previous studies the mean age was 39 similar to our study [6]. Predominance of females was noted in our study.
<20 20-29 30-39 40-49 50-59 60-69
In our study out of 150 cases 13% were malignant
and among malignant lesion most common was papillary carcinoma. In a study by EA Sinna et al [7] nodular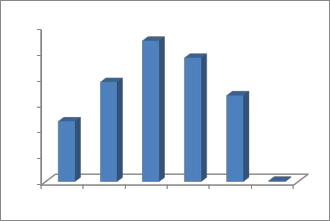
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 516
ISSN 2229-5518
hyperplacia represented majority of benign lesion (89.8%) while papillary carcinoma most frequent malignant lesion. In our study FNAC when compared with post operative pathological diagnosis showed good correlation in malignant nodules. Out of 18 cases, 17 cases correlated with FNAC report.
1. The commonest pathological entity observed in thyroid nodules in our study was colloid nodule. Among malignant nodule papillary carcinoma was the commonest. The highest incidence of thyroid nodule is seen in 30-39 age groups.
2. Very good correlation between FNAC and post operative pathology in malignant nodules.
1. Brander A, Vikinkoshi P, Nickel J, Kivisaari L.
Thyroid gland. US screening in random adult population.
2. Ezzat S, Sati, DA, Cain DR, Braunstein GD.
Thyroid incidentato mass prevalence by palpation and ultrasonography. Arch. Internal Medicine
1994; 154: 18; 38-40.
3. Toro L, Henoicbsen MD, Carl C. Rading MD ; Thyroid ultrasonography. Part 2: Nodules. Radiol. Clin. North. Am. 2011 May: 49 (3): 417-24.
4. Ross DS. Non palpable thyroid nodules managing an epidemic Jelin. Endocrinol. Metab. 2002; 87:
1930-40.
5. Rausch P, Nowels K. Jeffirey RB. Jr. Ultrasound graphically guided thyroid biopsy a review with emphasis on technique. J. Ultrasound. Med. 2001:
20: 79-85.
6. Ankush Dhanadia, Harshad Shah. Asutosh Dave.
Dept. of Radiodiagnosis. GU Shah, Medical College. Ultrasonographic and FNAC correlation of thyroid lesions. March 2014; Vol. 69 No. J. 75-80.
7. EA Sinna, N Ezzat. Diagnostic accuracy of fine needle aspiration cytology in thyroid lesions. Journal of Egypt National Cancer Centre. Vol. 24: Issue 2, 2012 June 63-
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014
ISSN 2229-5518
517