International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1112
ISSN 2229-5518
Subcutaneous Lipoma of The Tip of The Nose; A Rare
Presentation
Bhushan Kathuria, SPS Yadav, Vineet Panchal, Viresh Arora
Abstract; Lipoma are by no means uncommon tumour. They are rarely reported in the nose and paranasal sinus. W e report an unusual case of subcutaneous lipoma of the tip of nose in a 18 year old female which has not been reported in english literature. This was excised using open rhinoplasty approach. Follow up of one year revealed no recurrence. Differential diagnosis and management strategy is discussed.
Key words; Lipoma, Tip of nose, open rhinoplasty.

Introduction; Lipoma is the most common benign mesenchymal soft tissue tumour of mature adipocytes out of which 13-20% occur in head and neck region.1 These tumour are very rare in sinonasal tract. Lipoma of face and scalp are rarely reported, comprising less than 2% of lipoma.2 In literature lipoma of the oesophagus, colon, pharynx, larynx, trachea, nasal cavity and paranasal sinuses have occasionally been reported. In this article we describe a rare case of subcutaneous lipoma present at tip of the nose which to best of our knowledge is the first such case reported, however a case of fibrolipoma of tip of nose is reported in literature.3 Only one case of subcutaneous lipoma of vestibule of nose is reported in english literature.4
Case report: A 18 year female patient presented to us complaining of swelling over tip of nose for 10 years with no additional complains. It appeared insidiously and enlarged gradually without any pain. There was no history of similar swelling in the head and neck region as well as any other site of the body. Her medical and family history revealed nothing abnormal.
Examination on revealed a diffuse swelling of size 2x1.5 cm in diameter with smooth surface, non-tender, non-reducible and soft to firm in consistency over the tip of the nose. There was no discoloration, erythma or other sign of inflamation. The tip of the nose was broad in appearance. Nasal septum was in the midline and the nasal mucosa was normal. Clinical diagnosis of cyst/lipoma was entertained. USG swelling revealed hypogenic lesion of size approx. 2x 1.7 cm in subcutaneous plane of tip of nose. Fine needle aspiration & cytology revealed features of lioma. This was followed by surgical excision of swelling under local anaesthesia after obtaining a written informed consent.

Fig. 1
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1113
ISSN 2229-5518
An open rhinoplasty incision was given (Fig. 1) Swelling was dissected from the skin as well as as the underlying cartilage framework. It was found adherent to dorsal boarder of the septal cartilage as well as dome of both the lower lateral cartilages.
There was barely dissus The mass was excised and dome of lower lateral cartilages were approximated with vicryl 4-0 by interdomal suture technique. A columellar strut was put and secured to both medial crura. The incision was sutured with 4-0 prolene. The post operative period was uneventful.
Histopathology report of the excised mass confirmed the preoperative diagnosis of lipoma which revealed mature adipocytes with minimal variation in size of adipocytes dissected by thin fibrous septa.(Fig.2)
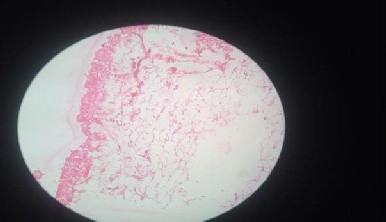
Fig.2 Photomicrograph of the specimen(H&E stain 400X magnification) showing
Discussion
Lipomas are well circumscribed, slow growing, benign tumors composed of mature fat cells, The peak incidence is in the fifth and sixth decades of life, and they are rare under the age of 20 years. However, present case was only 18 years of age. Histologically, lipomas are classified as simple lipoma or its variants such as: fibrolipoma, angiolipoma, chondroid lipoma, myolipoma, spindle cell lipoma, lipomatosis, sialolipoma, hipernoma, pleomorphic lipoma, myxoid and atypical lipoma.5,6
Lipoma are freely mobile in relation to the surrounding tissues, however this was not so in the present case as it was adherent to
dome of both lower lateral cartilages. They may clinically have a semi-lucent yellow color because of the thin overlying epithelium. In the present case there was no such discoloration as it was lying below the skin & not the mucosa. In some cases it is possible to observe the superficial blood vessels as well. The consistency of this lesion varies from soft to firm, depending on the quantity and distribution of fibrous tissue and depth of the Tumour7. The clinical differential diagnosis of lipoma of the tip of the nose include fibroma, fibrolipoma, other variants of lipoma and cysts. These are usually composed of mature adipocytes surrounded by a thin fibrous capsule.8 Fibrolipoma is characterized by mature adipose tissue interspread with band of broad or fascicles of dense connective tissue fiber within the capsule and have greater proliferative activity than other variants. While liposarcoma is extremly rare, but this entity cannot be distinguished from its benign counterpart by clinical examination only. So, differential is based on lack of lobular architecture, prominent fibrosis and multivacuolated adipose cells with indented nuclei(lipoblast) which are typical in liposarcoma. Therefore accurate histological examination is mandatory.9 Several lipomas of the nasal cavity and paranasal sinuses have been previously reported. Most of these lipomas occur in paediatric patients either as solitary lesions.10-11 or as part of a syndrome.12 Histopathological examination of the excised tissue is a gold standard investigative procedure along with consultation with pathologist for correct diagnosis and to exclude any degree of malignant transformation into liposarcoma. It is essential to document new cases which should be followed up carefully so that accurate, better treatment modalities could be drawn for future.
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 1114
ISSN 2229-5518
6
References
1 Fregnani ER, Pires FR, Falzoni R, et al. Lioma of the oral cavity: clinical findings, histological classification and proliferative activity of 46 cases. Int J Oral Maxillofac Surg. 2003 Feb; 32(1):49-53.
2 Truhan AP, Garden JM, Caro WA, et al. Facial and scalp lipomas: case report and study of prevalence. J Dermotol Surg
Oncol. 1985;11(10):981-4.
3 Jung SN, Shin JW, Kwon H and Yim YM. Fibrolipoma of the Tip of the Nose. J Craniofac Surg.2009;20(2):555-6.
4 Abulezz T, Allam K. Nasal subcutaneous lipoma, a case report. Rhinology.2008;46:151-2.
5 Gneep DR. Diagnostic surgical pathology of head and neck. Philadelphia:WB Saunders; 2001:191-4.
6 Weiss SW, Goldblum JR. Benign lipomatous tumours. In: Enzinger and Weiss’s soft tissue tumours. St.Louis: Mosby;
2001;4:571-639.
7 Bandeca MC, de Pedua JM, Nadalin MR, et al. Oral soft tissue lipomas: a case series. J Can Dent Assoc. 2007;73(5):431-4.
8 De Visscher JG. Lipomas and fibrolipomas of the oral cavity. J Maxillofac Surg. 1982; 10(3):177-81.
9 Capodiferro S, Maiorano E, Scarpelli F. et al. Fibrolipoma of the lip treated by diode laser surgery: a case report. J Med
Case Reports. 2008;42:301. doi: 10.1186/1752-1947-2-301.
10 Preece J.M, Kearns D.B, Wickersham J.K, et al. Nasal lipoma. J Laryngol Otol. 1988;102: 1044-6.
11 Chmielik M, Stelegowska-Piorkowska D. Congenital nasal lipoma. Otolaryngol Pol. 1993. 47: 274-8.
12 Hollis L.J, Bailey C.M, Albert D.M, Hosni A. Nasal lipomas presenting as part of a syndromic diagnosis. J Laryngol
Otol. 1996; 110: 269-71.
Address for correspondence: Bhushan, Junior resident, Department of Otolaryngology, Head & Neck Surgery, Post Graduate
Institute of Medical Sciences, Rohtak (India)
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014
ISSN 2229-5518
Email id. Kathuriabhushan56@gmail.com
1115
I£ER 2014 http://WWW.ISer.org