International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 263
ISSN 2229-5518
Obesity of Primary School Children: A Cross- sectional Study in Bangladesh
Mohammad Ohid Ullah, Md. Abu Hasan, Mohammad Mahmudur Rahman, Abul Hasan Chowdhury, Novel Chandra Das, Md
Jamal Uddin, Mohammed Taj Uddin
Abstract— The prevalence of obesity and overweight, as a most serious public health problem, has been studied in Bangladesh but not based on a particular city outside of Dhaka. Sylhet, as a developing city, is presumed that it is at risk of holding obese children. So our aim was to uncover the health status of primary school going children of this city and to identify the factors liable to renovate the obesity problem. We collected height, weight and other relevant information from 300 children through a house-based purposive survey. Descriptive analysis and Principal Component Analysis (PCA) have been applied to analyze the data. Among 300 children (aged 5-14 years) we have found 76% are healthy weight, 13.3% overweight, 5.3% underweight and 5.3% obese, where girls have slightly higher obesity rate than boys. Mothers’ occupation, family income, general food intake, computer game and outside-sports are the influential factors of obesity. Although, the level of obesity is not so high, proper steps should be taken to minimize the existing rate through developing both school and family based programs; otherwise the problem could be severe in the future. Taken together, we conclude that the study may help to develop the awareness about the childhood obesity and its associated diseases.
Index Terms— Obesity, Children, Primary school, Cross-sectional study, Factors, Body Mass Index, Principal Component Analysis.
—————————— ——————————
1 INTRODUCTION
hildhood obesity is one of the most serious public health challenges of the 21st century. According to
the World Health Organization (WHO), this problem is universal and is gradually affecting many low- and middle-income countries. Its effect can be seen particularly in urban settings [1]. It has been observed that the prevalence of childhood obesity [2] is approaching epidemic proportion in many economically developed countries; mainly USA, Canada, Australia and several European countries [3]. However, its prevalence in developing countries cannot be ignored. Furthermore according to WHO, the increasing rate of obesity is often faster in developing countries than in the developed countries. The prevalence of obesity has reached so high that a fifth of all global deaths today can be attributed to overweight or obesity [4]. It has been found that overweight and obesity in childhood and adolescence is associated with increased risk of both premature mortality and adult morbidity, particularly a cardio metabolic morbidity [5]. The morbidity rate which is linked with childhood obesity is same in both developed and developing countries. Obesity is also associated with hypertension, type 2 diabetes, asthma, sleep apnea, and reduced exercise capacity [6].
A recent study conducted by International Center for
————————————————
• Mohammad Ohid Ullah, PhD is currently serving as an Associate Professor in the Dept. of Statistics, Shahjalal University of Science and Technology, Sylhet, Bangladesh. E-mail: ohidullah@gmail.com, ohid-sta@sust.edu
• Md. Abu Hasan, Mohammad Mahmudur Rahman, Abul Hasan Chowdhury, and
Novel Chandra Das are currently pursuing MS program in the Dept. of Statistics,
Shahjalal University of Science and technology, Sylhet, Bangladesh. Md Jamal Uddin, PhD is currently serving as an Assistant Professor in the Dept. of Statistics, Shahjalal University of Science and Technology, Sylhet, Bangladesh and Mohammed Taj Uddin, PhD is currently serving as a Professor in the Dept. of Statistics, Shahjalal University
Diarrhoeal Disease Research, Bangladesh (ICDDR,B) reveals that 10% of children aged 5-18 years in Bangladesh are overweight in urban areas, while 4% are obese [7]. Previous study reveals that the percentage of overweight in Bangladesh was 1.1% among children aged
0-5 years in 1996-97 [8]. Though not all obese infants
become obese child and not all obese children become obese adults, some study suggest that obesity at early childhood will stick with throughout the life span of an individual [9,10]. Furthermore, there is evidence of a close relation between adolescent obesity and increased risks for health in adult life [11, 4]. An intervention study was also done by [12] for preventing childhood obesity. Several studies suggest that there is a close relation between fast-food consumption and total energy intake or bodyweight in adolescents and children [13-15] and these are considered as the major causes of moving toward childhood obesity in an epidemic situation in both developed and developing countries [16]. High intakes of sugar sweetened beverages, breakfast skipping, lack of physical activity, high levels of ‘screen time’ (e.g. watching TV or playing e-games), and lack of sleep [17,
18, 19] are associated with overweight and obesity among
school-aged children [20-22]. In developing countries, upper socioeconomic group has been suffering from obesity due to adoption of an increasingly Western lifestyle [23-25]. Obesity is clearly a complex problem for the individual as well as society. It is really important to approach obesity not only as a clinical problem but also as a public health problem [26].
Although Sylhet is a small city as compared to the capital
city of Bangladesh, it has been described as one of the wealthiest cities in the country. Several researches about childhood obesity have been performed based on Dhaka
of Science and Technology, Sylhet, Bangladesh.
IJSER © 2014
http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 264
ISSN 2229-5518
city or overall country [27], but in our knowledge this research findings are new for solely in Sylhet region. This region’s economy is mainly based on foreign remittance and the money is mainly sent by expatriates of Sylhet living abroad, particularly in the United Kingdom, where the majority of the migrated Bangladeshi community originates from Sylhet. There is a tendency of practicing western lifestyle in this region and this apparently leads to an increased risk of childhood obesity. Therefore, we aimed to know the health status of primary school going children of this city and to identify the factors that are liable for obesity. This study will help both the policymakers and health professionals to overlook the real situation of this very important phenomenon for overcoming future threat.
2 MATERIALS AND METHODS
Cross-sectional data were obtained by house to house visit from 300 selected p r i ma r y - s c h ool students who are studying primary school in Sylhet City. The sample sizes were determined by purposive sampling and data were collected during February to March in
2014. Children’s height, weight were measured using valid equipments and other information were obtained by asking them as well as their parents. We adequately informed each participant about the aims and methods of our study as well as our institutional affiliations. We collected data from participants with written consent from the guardians. Th e r e s e a r c h p r ot oc ol of t h e s tu d y w a s a pp r o v e d b y th e c o m m i tte e o f th e U n i v ersi t y R e sea rc h C en t er o f Sh ah j al a l U ni v e r s i t y o f S c i e nc e a nd T e c hno l o g y , Ba n g l a de s h .
Descriptive analysis of this study was done by SPSS. Because of purposive sampling in which observations were not random, we did not apply linear regression to answer our research question. In that case, we performed Principal Component Analysis and that was done using FactoMineR package [28] in R.
3 RESULTS
3.1 Descriptive Analysis
Based on Body Mass Index (BMI) to screen for overweight and obesity in children and teens as recommended by Center for Disease control and Prevention (CDC) and the American Academy of Pediatrics (AAP) (Table 1) [29], we found that BMI less than 12 refers underweight, 12-18 refers healthy weight,
18.01-21 overweight and more than 21 is obese.
Table 1. BMI group based on weight status
Weight status category | Percentile range ( aged between 2-20) [29] | BMI group (for our data) |
Underweight | Less than the 5th percentile | <12 |
Healthy weight | 5th percentile to less than the 85th percentile | 12-18 |
Overweight | 85th to less than the 95th percentile | 18.01-21 |
Obese | Equal to or greater than the 95th percentile | >21 |
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 265
ISSN 2229-5518
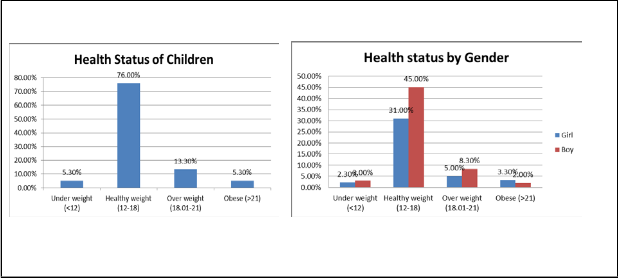
The data comprises 58% and 42% of male and female respectively. In our investigation we found that 5.3% of children are underweight, 76% healthy weight and 5.3% obese [Fig. 1A]. Girls (3.3%) are more obese than boys (2%). Boys have the higher percentage (45%) in healthy weight group than girls (31%). In overweight and underweight groups, boys are of higher proportions as well [Fig. 1B]. Father’s occupation does not show any effect on children’s obesity situation. We found that 85% mothers are housewives and in this group 5.5% children are underweight, 77.3% are healthy, 12.9% are overweight and noticeably just 4.3% are obese.
Family income is considered as one of the most important factors among others. We found that obese and healthy weight children’s are clustered into middle income society while the family incomes of overweight children are much higher than that of underweight groups. We observed that 90% children take fast food. We also found that average Height, Weight, Waist size and Arm size of the obese group are larger than all other groups (Table 2). It shows average waist size and arm size increases as BMI increases.
(A) (B)
Fig. 1. (A) Health status of children. (B) Health status of children by Gender.
Table 2. Average and standard deviation (SD) of Height, Weight, Waist size and Arm size of different health status.
BMI Group | Height (m) | Weight | Waist size | Arm size |
BMI Group | Mean(SD) | Mean(SD) | Mean(SD) | Mean(SD) |
<12 (underweight) | 1.18(.10) | 16.22(2.9) | 50.63((3.6) | 14.81(.9) |
12-18 (healthy weight) | 1.26(.12) | 23.74(5.6) | 58.65(6.0) | 17.64(2.1) |
18.01-21 (overweight) | 1.37(.09) | 35.93(4.4) | 70.65(10.8) | 22.21(1.8) |
>21(obese) | 1.39(.10) | 44.20(7.3) | 80.03(8.5) | 24.09(2.7) |
3.2 Principal Component Analysis
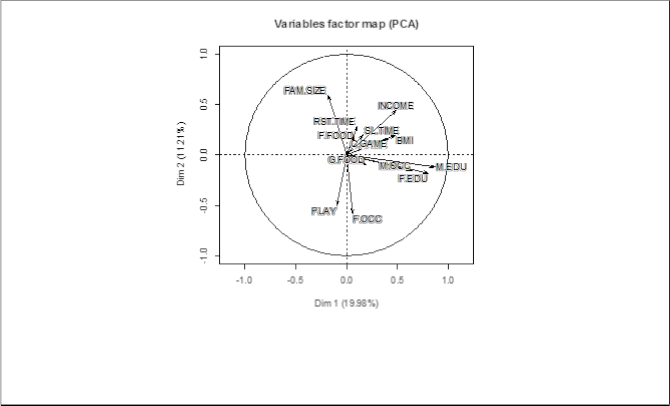
To find out the associated factors of BMI, we used FactoMineR package in R. In this study we considered total 13 potential associated factors (Table 3) with BMI. The factors which have positive loading of Dim1 indicate the factors located on 1st and 4th quadrant. Observing the
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 266
ISSN 2229-5518
loading values (Table 3) of different dimensions and correlation circle (Fig. 2), we found that income and computer game are the factors having high positive association with BMI. These findings show that children whose parents have more income and who play the computer game are more obese than others. General food ((meat, milk, egg, potato) = 1, (vegetable, fish, pulse)=0 ),
Rest after time (yes=1, no=0), Fast food (yes=1, no=0), Sleeping time, Father education, Mother education, Mother occupations are also associated with BMI. Children, who are eating fatty food like meat, egg, and potato, have higher BMI than who do not take fatty food frequently.
Table 3. Loadings of the different factors
Factors | Details | Dim1 | Dim2 |
M.EDU | Mother education | 0.873479 | -0.11573 |
F.EDU | Father education | 0.806504 | -0.18023 |
M.OCC | Mother occupation | 0.641753 | -0.15328 |
INCOME | Family Income | 0.490595 | 0.44407 |
BMI | Body mass index | 0.483253 | 0.199252 |
C.GAME | Computer game | 0.413582 | 0.16097 |
G.FOOD | General food | 0.191581 | -0.09362 |
SL.TIME | Sleeping time at night | 0.161107 | 0.200541 |
RST.TIME | Rest time after lunch | 0.105232 | 0.290658 |
F.FOOD | Fast food | 0.077298 | 0.202362 |
F.OCC | Father occupation | 0.059032 | -0.58311 |
PLAY | Play outside | -0.09479 | -0.50519 |
FAM.SIZE | Family | -0.1846 | 0.595736 |
Fig. 2. Variable factor map or correlation circle or loading plot. It shows the association among the factors of obesity. Longer the vectors indicate more influential and the vectors that are close of each other with same direction indicate highly positive association. Vectors that are opposite direction are showing negative association and the vectors that are almost 90 degree angle are showing no association. First principal component shows around 20% of the variation in the dataset and 2nd one show around 11% of the variation of the dataset.
Children, who take a rest after lunch, go to bed late at
night, play the computer game and take fast food (snacks bar, burger etc.) are more obese than others. Usually
higher educated parents have higher income and they
avail to buy fatty food like fast food and meat, therefore their children are fattier than others. This means educated
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 267
ISSN 2229-5518
parents need to have more nutritional knowledge so that they can practice healthier food. Another point could be that a mother with a job might not have time to take care their kids properly.
We also found Play outside (yes=1, no=0) is slightly negatively associated with BMI, suggesting that children who do not play outside are more obese. Father occupation and family size show almost no association with BMI.
4 DISCUSSION
The prevalence of obesity [2], however, around the world is increasing at an alarming rate; in Bangladesh its rate is not as much higher as other developing countries. Sylhet is a financially developed city and many people are capable of afford a western lifestyle, in view of the fact that many people of this city are living in the UK and other developed countries. Several studies [2, 27, 30-32] have been conducted about childhood obesity in Bangladesh; however to the best of knowledge none has been conducted based on Sylhet city. We found that the percentage of obese children is 5.3% and overweight is
13.3% who are belonging to the age group 5-14 years.
Earlier research indicates that the prevalence of obesity and overweight differ between girls and boys and is significantly higher among youth from lower socioeconomic background all over the world [33-37]. In a similar pattern, it was observed in Sylhet city that obesity and overweight rate vary on gender, where girls are more obese than boys. Some studies [38-39] have been suggested that the prevalence rate of obesity and overweight is high in lower socioeconomic groups while other suggest in higher economic group. However, we found that it is high on higher income group. As girls are more obese than boys, more concentration should be given to the girls because they often stay at home and do not get enough facility like boys to play or do other outdoor physical activity.
It is observed that, mother’s occupation influences on child health. Housewife mothers have enough time to take care their children and give proper care to them; as a result, the proportion of obese children belong to housewife mothers are very few. So mothers, who work outside of the home, should pay more attention to their children’s health.
Sleeping time may cause the problem, and it is highly associated with BMI. It may be considered that instead of sleeping, those obese children give more time on desk activity like playing computer games, watching TV etc. [19] which keep children out of sleeping particularly on day time. We should inspire children to do some physical
activity like walking regularly either on free time or on the way of going school regularly.
Lower socio-economic status tends to be associated with obesity for adults. Even as the same relationship has been observed for children, the association is usually not as strong and results are inconsistent [40-42]. Another study found that, children and adolescents in middle-income households were more likely to be obese than those in high income households [43]. Similar result has been seen in our study that children of middle income family belong to healthy weight group as family income is highly associated with BMI. This means children who belong to high income family are more obese. The main problem is that the average income of the overweight group is much higher than other groups, which might cause the prevalence of obesity to epidemic in the future. On the other hand, children from lower income society suffer from underweight problem, due to lack of nutritious food and other consequences. In fact, rich families are not always aware of their children’s health. They feed them luxurious food like fast food, but keep them away from physical activity and consequently the children from this class are more chance to be obese.
Playing outside, a very potential source of physical activity, keep tracking children on good health, while we have evidence that playing any kinds of games like computer games (video games or indoor games) sometimes causes really bad effect on their health. Low levels of physical activity are associated with high risk of childhood obesity [44]. Some studies have been found that physical activity protects against childhood obesity [45], while others have not found such a relationship [46]. Our results show that children who do not play outside are more obese. Playing regularly outdoor games like cricket, football and many others childish games with proper physical movement keep children safe from becoming obese or overweight.
The rise in consumption of fast food might have particular relevance to the childhood obesity epidemic in developed and developing nations. Results of several studies [12-14] suggest an association between fast-food consumption and total energy intake or bodyweight in adolescents and adults. The consumption of fast food on obese or overweight group and healthy weight group children’s are respectively high. Though it has been suggested from several studies that energy-dense foods, high fat and high sugar snacks, affordable and easily available fast foods have contributed immensely to the epidemic of obesity [47].
Young people who eat food like meat, milk, egg and potatoes (French fries) were likely to be more overweight/obese than those who eat pulse, fish and vegetables more frequently [39]. Children’s weights also
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 268
ISSN 2229-5518
vary with consumption of fast-food. In both sexes, the frequency of consumption of vegetables, as well as dairy products, decreased the risk of becoming obese or overweight. Taking proper foods like vegetables, meat, fish, egg, milk, those contains proper nutrients and vitamins, support children to maintain a good and healthy life. The tendency of taking rest after lunch was found to have a positive association with BMI. The association between educational status of maternal and childhood obesity was also significant in Dhaka city and the level of childhood obesity among school children of the affluent society is very high [48]. In Sylhet city maternal education also show a positive association with BMI, indicates that children from lower educated mothers are less obese than higher educated mothers.
Obesity of urban children was positively associated with family income, expenditure on food, increased intake of energy, parental obesity, and duration of television watching [43]. From our study, we can summarize that, the prevalence of obesity is much lower as compared to Dhaka, but the overweight rate is somewhat alarming, it could be much higher in the future. Girls are more obese than boys and children from housewife mothers are healthier than others.
The coexistence of underweight and overweight poses a
challenge to public health programs [49], however, this
city has even showed better result in this perspective; whereas other urban cities of developing countries including Bangladesh are vulnerable in this situation. The level of obesity is going to increase in the future due to unplanned rapid urbanization, small school houses, lack of playground and insecure playground, more home entertainment like television and video games, excessive homework or extra coaching after school hour.
5 CONCLUSION
Although the extent of obesity has been found less as compared to other parts of this country, in the future it may be a great problem if proper consideration is not taken as the overweight rate is very high. We should increase the awareness level of parents, including existing family members, about the horrific effect of obesity and overweight. School or family based programs that support physical activity, modification of dietary intake, and decrease of inactive behaviors may help to reduce childhood obesity. This research work may help the policymaker to take proper steps for public health - especially children in the Sylhet city of Bangladesh. [10] Serdula MK, Ivery D, Coates RJ, Freedman DS, Williamson DF, Byers T (1993) Do obese children become obese adults? A review of the literature. Prev
Med 22: 167–177.
[11] Power C, Lake JK, Cole TJ (1997) Measurement and
Strategies can be recommended for other developing countries in the world as well.
ACKNOWLEDGMENTS
The authors wish to thank The Director of The Research Centre, Shahjalal University of Science and Technology (SUST), Sylhet, Bangladesh for providing funds to conduct this study. The authors also wish to thank Prof. Dr. Shahidul Islam, Dept. of Statistics, SUST, Bangladesh for his valuable comments.
REFERENCES
[1] World Health Organization: Global Strategy on Diet, Physical Activity and Health. Available: [http://www.who.int/diet
physicalactivity/childhood/en/]. Accessed 24 May
2014.
[2] Sultan K, Habiba T (2008) Prevalence of overweight
and obesity in infancy. Bangladesh Med Res Counc
Bull 34: 69–70.
[3] Wang Y, Lobstein T (2006) Worldwide trends in
childhood overweight and obesity. Int J Pediatr Obe
1: 11-25.
[4] Must A, Strauss RS (1999) Risks and consequences of childhood and adolescent obesity. Int J Obes Relat Metab Disord 23(Suppl 2):S2–S11.
[5] Reilly JJ, Kelly J (2011) Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes (Lond) 35: 891–898.
[6] Suskind R, LeWinter-Suskind L (2006) Proceeding of
the 8th CCDM on Childhood Obesity: A Growing
Nutritional Threat in the Developing World: 8
February 2006; Sasakawa Auditorium.
[7] ICDDR,B. Available:
[http://www.icddrb.org/media- centre/media-releases/doc_download/7761- new-icddrb-study-reveals-that-10-out-of- every-100-children-living-in-an-urban-area- in-bangladesh-are-overweight-and-4-are- obese]. Accessed on 25 May 2014.
[8] De Onis M, Blossner M (1998) Prevalence and trends of overweight among preschool children in developing countries. Am J Clin Nutr 72: 1032–1039.
[9] Prentice AM (1998) Body mass index standards for children are useful for clinicians but not yet for epidemiologists. Br Med J 317: 1401-02.
long term health risks of child and adolescent fatness. Int J Obes Relat Metab Disord 21:507–526.
[12] Campbell K, Waters E, O’Meara S, Summerbell C. Interventions for preventing obesity in children. The Cochrane library, issue 1,
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 269
ISSN 2229-5518
2002<www.cochranelibrary.com> (Version current at
April 22, 2002).
[13] French SA, Story M, Neumark-Sztainer D, Fulkerson JA, Hannan P (2001) Fast food restaurant use among adolescents: associations with nutrient intake, food choices and behavioral and psychosocial variables. Int J Obesity 25: 1823–1833.
[14] French SA, Harnack L, Jeffery RW (2000) Fast food restaurant use among women in the Pound of Prevention study: dietary, behavioral and demographic correlates. Int J Obes Relat Metab Disord 24: 1353–1359.
[15] Binkley JK, Eales J, Jekanowski M (2000) The relation between dietary change and rising US obesity. Int J Obesity 24: 1032–1039.
[16] Ebbeling CB, Pawlak DB, Ludwig DS (2002)
Childhood obesity: public-health crisis, common
sense cure. The Lancet 360: 473–482.
[17] Cappuccio FP, Taggart FM, Kandala NB, Currie A,
Peile E, Stranges S, Michelle A (2008) Meta-analysis of short sleep duration and obesity in children and adults. Sleep 31:619–626.
[18] Chen X, Beydoun MA, Wang Y (2008) Is sleep duration associated with childhood obesity? A systematic review and meta-analysis. Obesity (Silver Spring) 16:265–274.
[19] Brug J, van Stralen MM, Te Velde SJ, Chinapaw MJ,
De Bourdeaudhuij I, Lien N, Bere E, Maskini V, Sing AS, Maes L, Moreno L, Jan N, Kovacs E, Lobstein T, Manios Y: (2012) Differences in Weight Status and Energy-Balance Related Behaviors among Schoolchildren across Europe. PLoS One 7(4): e34742.
[20] Maffeis C (2000) Aetiology of overweight and obesity in children and adolescents. Eur J Pediatr 159(Suppl
1): S35–S44.
[21] Rennie KL, Johnson L, Jebb SA (2005) Behavioral determinants of obesity. Best Pract Res Clin Endocrinol Metab 19: 343–358.
[22] Swinburn BA, Caterson I, Seidell JC, James WP (2004) Diet, nutrition and the prevention of excess weight gain and obesity. Public Health Nutr 7:123–146.
[23] Martorell R, Khan LK, Hughes ML, Grummer- Strawn LM (1998) Obesity in Latin American women
and children. J Nutr 128: 1464–1473.
[34] Gordon-Larsen P, Adair LS, Popkin BM (2003) The relationship of ethnicity, socioeconomic factors, and overweight in US adolescents. Obes Res 11: 121–129.
[35] Sallis JF, Prochaska JJ, Taylor WC (2000) A review of correlates of physical activity of hildren and adolescents. Med Sci Sports Exerc 32:963–975.
[36] Te Velde SJ, De Bourdeaudhuij I, Thorsdottir I, Rasmussen M, Hagströmer M, Klepp KI, Brug J (2007)
[24] Doak C, Adair L, Bentley M, Fengying Z, Popkin B (2002) The underweight/overweight household: an exploration of household sociodemographic and dietary factors in China. Public Health Nutr 5: 215–
221.
[25] Popkin BM (2002) An overview on the nutrition
transition and its health implications: the Bellagio
meeting. Public Health Nutr 5: 93–103.
[26] Christakis NA, Fowler JH (2007) The Spread of
Obesity in a Large Social Network over 32 Years. N Engl J Med 357: 370-9.
[27] Rahman S, Islam MT, Alam DS (2014) Obesity and
overweight in Bangladeshi children and adolescents:
a scoping review. BMC Public Health 14: 70.
[28] De Tayrac M, Le S, Aubry M, Mosser J, Husson F (2009) Simultaneous analysis of distinct Omics data sets with integration of biological knowledge:
Multiple Factor Analysis approach. BMC Genomics
10: 32.
[29] Centers for Disease Control and Prevention.
Available:
[http://www.cdc.gov/healthyweight/assessin
g/bmi/childrens_bmi/about_childrens_bmi.h tml]. Accessed 30 May 2014.
[30] Mohsin F, Tayyeb S, Baki A, Sarker S, Zabeen B, Begum T, Azad K, Nahar N: (2010) Prevalence of obesity among affluent school children in Dhaka. Mymensingh Med J 19: 549–554.
[31] Rahman SMM, Akter BMD, Siddiqui MZA (1998)
Prevalence of childhood Obesity in Dhaka city. Mymensingh Med J 7(1):3–6
[32] Das SK, Chisti MJ, Huq S, Malek MA, Vanderlee L,
Salam MA, Ahmed T, Faruque ASG, Al-mamun A (2013) Changing trend of overweight and obesity and their associated factors in an urban population of Bangladesh. Food Nutr 4: 678–689.
[33] Haug E, Rasmussen M, Samdal O, Iannotti R, Kelly
C, Borraccino A, Vereecken C, Melkevik O, Lazzeri G, , Giacchi M, Ercan O, Due P, Ravens-Sieberer U, Currie C, Morgan A, Ahluwalia N (2009) Overweight in school-aged children and its relationship with demographic and lifestyle factors: results from the WHO-Collaborative Health Behaviour in School- aged Children (HBSC) study. Int J Public Health 54 (Suppl 2): 167–179.
Patterns in sedentary and exercise behaviors and
associations with overweight in 9–14-year-old boys and girls–a cross-sectional study. BMC Public Health
7: 16.
[37] Wang Y, Liang H, Tussing L, Braunschweig C, Caballero B, Flay B (2007) Obesity and related risk factors among low socio-economic status minority students in Chicago. Public Health Nutr 10: 927–938.
[38] Sultana S (2010) Prevalence and risk factor of
childhood overweight and obesity in primary school children of Dhaka city, Master’s thesis. University of
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 12, December-2014 270
ISSN 2229-5518
Oslo: Faculty of Medicine.
[39] Rahman SMM, Kabir I, Khaled MA, Bhuyan MAH,
Rashid HA, Malek MA, Khan MR (2002) Prevalence and Determinants of Childhood Obesity in Dhaka City. In Proceedings of 10th ASCON. Abstract no.:173, Dhaka.
[40] Guillaume M, Lissau I. Epidemiology.In: Burniat W,
Cole TJ, Lissau I, Poskitt ME (2002) Childhood and Adolescent Obesity: Causes and Consequences, Prevention and Management. Cambridge. Cambridge University Press pp.28-49.
[41] Hill AJ, Lissau I. Psychosocial factors. (2002) In:
Burniat W, Cole T, Lissau I, et al., eds. Adolescent
Obesity: Causes and Consequences,
Prevention and Management. Cambridge. Cambridge
University Press pp. 109-27.
[42] Willms JD, Tremblay MS, Katzmarzyk PT: (2003)
Geographic and demographic variation in the prevalence of overweight Canadian children. Obes Res 11(5): 668-673.
[43] Shields M (2006) Overweight and obesity among
children and youth. Health Rep 17(3): 27-42.
[44] Jimenez-Pavon D,Kelly J,Reilly JJ (2010) Association
between objectivity measured habitual physical activity and adiposity in children and adolescents: systemic review. Int J Pediatr Obese 5: 3-18.
[45] Tremblay MS, Willms JD (2003) Is the Canadian
childhood obesity epidemic related to physical inactivity? Int J Obes Relat Metab Disord 27(9): 1100-
1105.
[46] Lobstein T, Baur L, Uauy R (2004) Obesity in children and young people: A crisis in public health. Obes Rev 5(Suppl 1): 4-104.
[47] Bowman SA,Vinyard BT (2004) Fast food
consumption of U.S. adults: impact on energy and
nutrient intakes and overweight status. J Am Coll
Nutr 23: 163-168.
[48] Ahmed SMM, Islam MS, Razzaque A, Ahmed T (2007) Socioeconomic Differentials of Childhood Obesity among School Children in the Context of Affluent Society of Dhaka City. In Proceedings of 11th ASCON. Abstract: 104(125). Dhaka.
[49] Caballero B (2005) A Nutrition Paradox — Underweight and Obesity in Developing Countries. N Engl J Med 35: 15.
IJSER © 2014 http://www.ijser.org