International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 64
ISSN 2229-5518
Insulin Resistance, a surrogate marker, in type 2
Diabetes Mellitus
Suresh Kumar P
7th decade and beyond. The results showed that W HR has better correlation with IRS than the BMI. The control of diabetes was poor among nearly 2/3rd of the patients. 1/5th of males and 1/3rd of females had CAD. 67.21% of males and 71.19% of females had hypertension. 50% had positive family history of diabetes among 1st degree relatives. The lipid abnormalities were of lesser classical nature. More number of patients had abnormal LDL levels than having TGL or HDL abnormalities. 52.1% of males and 55% females had statistically significant lower calcium levels, whereas the uric acid levels were normal in more than 90%. The study also showed that the fasting insulin level is higher (90.4μU/ml for males and 72.3 μU/ml for females) and that it correlates well with the degree of insulin resistance. It may therefore be necessary to measure insulin level along with blood glucose and lipids in type 2 diabetes mellitus.
—————————— ——————————
ype 2 diabetes mellitus (T2DM) is an insulin resistant state associated with accelerated atherosclerosis, hypertension, dyslipidemia and abnormal vasomotor responses to insu- lin.[1] Insulin resistance is a hallmark of type 2diabetes that precede and predict the disease for several years.[2],[3] About
80-90% of all type diabetes coexists with insulin resistance which usually also precedes the first symptoms of the dis- ease.[4],[5] The prevalence of the insulin resistance syn- drome has varied markedly between different studies, most likely because of the lack of accepted criteria for the definition of the syndrome.[6] There is abundant evidence that insulin resistance is a treatable precursor of type 2diabetes and perhaps of cardiovascular disease as well.[2],[7] Risk factors for Type 2 diabetes and atherosclerotic vascular disease such as insulin resistance, dyslipidemia, and hypertension cluster together in affected individuals.[8] Insulin resistance is a common pathologic state in which target cells fail to respond to ordinary levels of circulating insulin. It is frequently asso- ciated with a number of diseases, including chronic infec- tion, human obesity, and type 2diabetes. Though insulin re- sistance could also be due to a defect in the binding of insulin to the receptor, it is mostly attributed to a post-binding defect in the hormone actions. In non-diabetic as well as diabetic sub- jects, insulin resistance is related to several cardiovascular risk factors, including hyperglycemia, dyslipidemia, hypertension, thrombophilia.[9],[10]
————————————————
• Suresh Kumar P is currently the Medical Director of Dr. Suresh‘s Di- abCare India, East West Cross Road, Nadakkavu, Kozhikkode, Kerala, In- dia-673011
Phone: +91 495 4012123
The patients for this study were drawn from the diabetic out- patient department at District Hospital, Manjeri, Malappuram, Kerala. They are screened for the presence of diabetes by checking the fasting and the post-prandial blood sugar levels according to the American Diabetes Association‘s new criteria for the diagnosis of diabetes mellitus.[11] Patients who were on insulin, other types of diabetes like Fibro-Calcific Pancreat- ic Diabetes (FCPD), Type-1DM (Insulin Dependent Diabetes Mellitus), Secondary Diabetes, Drug induced Diabetes, Gesta- tional Diabetes Mellitus (GDM) and patients with fasting blood sugar >300mg/dl were excluded from the study. After a run-in period of 3 months and a further 2 months for screen- ing for eligibility for inclusion in the study out of a total of 723 patients, 103 were selected for the final study. These patients who were not treated with insulin are further screened for the presence of hyper-insulinemia by measuring the blood level of fasting insulin concentration. Samples for the fasting blood Glucose, Lipids, Uric Acid, Calcium and fasting insulin levels were collected after at least 8 hours of overnight fasting. . Be- fore enrolling the patients for this study a consent letter was signed by each patient after explaining the details of the study to them. The Ethics Committee of the institution approved this project.
The Insulin resistance syndrome was diagnosed according to the NCEP ATP III definition.[12] A participant was deemed to have the syndrome when three or more of the following crite- ria were satisfied (Table 1)
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 65
ISSN 2229-5518
![]()
Table 1. Criteria for selection as insulin resistance syndrome
1) Waist circumference >102 cm in men and >88 cm in women
2) Triglyceride level >150mg/dL;
3) HDL cholesterol < 40mg/dL in men and < 50mg/dL in women
4) Blood pressure >130/85 mmHg or known treatment for hypertension
![]()
5) Fasting glucose level of > 110mg/dL or a known diabetic
HDL: High density lipoprotein
Since all participants in the study are already diagnosed as diabetics, only any two of the other 4 items (items 1 to 4) need to be positive to diagnose the presence of the syndrome.
Table 2. Mean values and Statistical significance of different parameters in diabetes with IR. | ||||||
Parameters | Male: N=61 | Female: N=59 | T TEST Significance P VALUE | |||
Mean | Mean | Male v/s Female) | Male v/s Normal Value | Female v/s Normal Value | ||
FBS | 158.08 | 155.27 | 0.784 | NV=<126, P=0.001‡ | NV=<126. P= 0.001‡ | |
PPBS | 235.21 | 230.50 | 0.715 | NV=<140, P=0.001‡ | NV=<140, P=<0.001‡ | |
F.Insulin | 92.10 | 72.28 | 0.056 | NV=<30, P=<0.001‡ | NV=<30, P=<0.001‡ | |
Chol | 195.92 | 206.47 | 0.144 | NV=<200, P=0.4581 | NV=<200, P=0.1669 | |
TGL | 153.42 | 149.03 | 0.777 | NV=<150, P= 0.741 | NV=<150, P=0.933 | |
HDL-C | 47.95 | 53.34 | 0.044‡ | NV=>40, P=<0.001‡ | NV=>50, P=0.0889 | |
LDL-C | 117.49 | 126 | 0.180 | NV=100, P=<0.001‡ | NV=100, P=<0.001‡ | |
UA | 6.11 | 5.55 | 0.718 | NR | ||
Ca | 8.13 | 8.14 | 0.954 | NV=8.5-10.5, P=< 0.001‡ | NV=8.5-10.5, P= 0.005‡ | |
FBS: Fasting Blood Glucose in mg/dL, PPBS: Post prandial Blood Glucose in mg/dL, F.Insulin: Fasting Insulin in mU/ml, Chol: Total Cholesterol in mg/dL, TGL: Triglycerides in mg/dL, HDL-C: High Density Lipoprotein Cholesterol in mg/dL, LDL-C: Low Density Lipoprotein Cholesterol in mg/dL, UA: Uric acid in mg/dL, Ca: Calcium in mg/dl NV: Normal Value, ‡ Significant |
The results of the present study are given in the table 2. The mean serum fasting insulin levels are higher in this study population than many other groups, indicating that we suf- fer from more insulin resistance than others. This study population has both high prevalence of insulin resistance and higher levels of fasting insulin levels. The diabetic dyslipidemia in the study population is of a lesser classical nature with the serum triglyceride levels lower than many others. Likewise, HDL levels are also found to be abnor- mal in only around 50% of the diabetics studied, where as the LDL cholesterol abnormalities were observed in a greater proportion (¾ to 4/5 ). It is observed that serum TGL was elevated and HDL cholesterol values were decreased. Low mean serum calcium levels among the diabetics, pre- dominantly among male diabetics and especially in the poorly controlled group, was observed. Mean serum calci- um levels among the diabetics, predominantly among male diabetics and especially in the poorly controlled group, was observed.
Several longitudinal studies of initially non diabetic indi- viduals have also found fasting hyper insulinemia to be predictive of future cardiovascular events.[13] In the presnt study 86.33%, (120 of the total 139) patients had hyper insu- linemia. Equating hyper insulinemia with insulin resistance as done in many other studies, gives us an estimate of insu- lin resistance among our T2DM patients, meaning that
86.33% of the total diabetics studied have insulin resistance
which is similar to the findings of Steven et al.[14] The TGL
value was significantly higher in the western studies, com-
pared to to the present study. Few studies which reported such higher values are Sangeetha et al.,[15] and Nystrom et al.,[16] Low HDL cholesterol levels are often accompanied by elevated triglyceride levels and the combination has been strongly associated with an increased risk of CHD. Elevated TGL reported from other geographical areas.
Figure 1: Mean values of different parameters in diabetes with IR.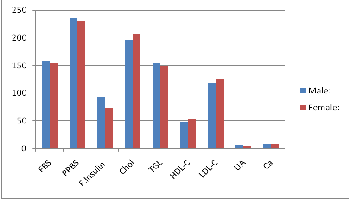
FBS: Fasting Blood Glucose in mg/dL, PPBS: Post prandial Blood Glucose in mg/dL, F.Insulin: Fasting Insulin in mU/ml, Chol: Total Cholesterol in mg/dL, TGL: Triglycerides in mg/dL, HDL-C: High Density Lipoprotein Cholesterol in mg/dL, LDL-C: Low Density Lipoprotein Cholesterol in mg/dL, UA: Uric acid in mg/dL, Ca: Calcium in mg/dl
IJSER © 2014 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 5, Issue 9, September-2014 66
ISSN 2229-5518
![]()
The cause of hypocalcaemia detected in the present study,
need further evaluation. It could either be due to intracellu- lar deficiency of Mg2+17 or probably due to the abnormal functioning of one of the least attended counter-regulatory hormones called PTH (parathormone) secondary to insulin resistance. From the study it can be concluded that IR is the cause of the biochemical alterations and the leading cause of secondary complications in T2DM.
![]()
[1] Mather, Kieren J., Helmut O. Steinberg, and Alain D. Baron. "Insulin re- sistance in the vasculature." The Journal of clinical investigation 123.3 (2013): 1003-1004.
[2] Kraemer, Fredric B., and Henry N. Ginsberg. "Gerald M. Reaven, MD: Demonstration of the Central Role of Insulin Resistance in Type 2 Diabe- tes and Cardiovascular Disease." Diabetes care 37.5 (2014): 1178-1181.
[3] Sales, Vicencia, and Mary-Elizabeth Patti. "The ups and downs of insulin resistance and type 2 diabetes: lessons from genomic analyses in hu- mans."Current cardiovascular risk reports 7.1 (2013): 46-59.
[4] Juhan-Vague I, Thompson SG and Jespersen J. Involvement of the hemo- static system in the insulin resistance syndrome: a study of 1500 patients with angina pectoris: the ECAT Angina Pectoris Study Group. Arterioscl. Thromb. 1993; 13: 1865 –1873.
[5] Hochholdinger, Franz, et al. "Novel membrane-targeted ERK1 and ERK2
chimeras which act as dominant negative, isotype-specific mitogen- activated protein kinase inhibitors of Ras-Raf-mediated transcriptional ac- tivation of c-fos in NIH 3T3 cells." Molecular and cellular biology 19.12 (1999): 8052-8065.
[6] Shulman, Gerald I. "Cellular mechanisms of insulin resistance." Journal of
Clinical Investigation 106.2 (2000): 171-176.
[7] Kahn, S. E. "The relative contributions of insulin resistance and beta-cell dysfunction to the pathophysiology of type 2 diabetes." Diabetologia 46.1 (2003): 3-19.
[8] Paneni, Francesco, et al. "Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part I." European heart jour- nal(2013): eht149.
[9] Batra, Ankur. Study Of Insulin Resistance And Inflammation In Relation To Various Degrees Of Blood Pressures In Adults-A One Year Cross Sec- tional Study. Diss. KLE University, Belgaum, Karnataka, 2013.
[10] Patil, Vikas S. A Comparative Study Of Insulin Resistance In Offsprings Of Type 2 Diabetes Mellitus And Non Diabetic Patients-A One Year Cross Sectional Hospital Based Study. Diss. KLE University, Belgaum, Karna- taka, 2010.
[11] American Diabetes Association. "Diagnosis and classification of diabetes mellitus." Diabetes care 36.Supplement 1 (2013): S67-S74.
[12] Bener, Abdulbari, et al. "Prevalence of Metabolic Syndrome According to
ATP III and IDF criteria: A population based study." QNRS Reposito- ry 2011.1 (2011).
[13] Steven E. Stern, Ken Williams, Eleuterio Ferrannini, Ralph A. DeFronzo,
Clifton Bogardus and Michael P. Stern. Identification of Individuals With
Insulin Resistance Using Routine Clinical Measurements Diabetes. 2005;
54(2): 333 - 339
[14] Reaven GM, Chen YD, Jeppesen J, Maheux P and Krauss RM. Insulin resistance and hyperinsulinemia in individuals with small, dense low density lipoprotein particles. J. Clin. Invest. 1993; 92: 141 – 146
[15] Sangeeta R. Kashyap, Linda J. Roman, Jennifer Lamont, Bettie Sue S.
Masters, Mandeep Bajaj, Swangjit Suraamornkul, Renata Belfort, Rachele Berria, Dean L. Kellogg, Jr., Yanjuan Liu and Ralph A. DeFronzo. Insulin Resistance Is Associated with Impaired Nitric Oxide Synthase Activity in Skeletal Muscle of Type 2 Diabetic Subjects. J. Clin. Endocrinol. Metab.
2005; 90: 1100 – 1105
[16] Lamarche B, Moorjani S, Cantin B, Dagenais GR, Lupien PJ, Despres J P. Associations of HDL2 and HDL3 subfractions with ischemic heart disease in men: prospective results from the Quebec Cardiovascular Study. Arterioscler. Thromb. Vasc. Biol. 1997; 17: 1098 – 1105.
[17] Junji Takaya, Hirohiko Higashino and Yohnosuke Kobayashi.
Intracellular magnesium and insulin resistance. Magnesium Research.
2004; 17(2): 126 – 136.
IJSER © 2014 http://www.ijser.org