International Journal of Scientific & Engineering Research Volume 2, Issue 9, September-2011 1
ISSN 2229-5518
Automated Learning in Medical Sensor System
Ayoni Mukherjee, Sanjit Setua
Abstract - Automated learning in medical sensor system for health care monitoring application is presented in this paper. We worked mainly on cardiology and have tried to integrate the benefits of medical instruments of the said domain. We have used multi-disciplinary concept of learning from different domains like philosophy, sociology , psychology , education apart from computer science. The system uses the concept of expert system , though it overcomes the limitations of any traditional rule-based expert system. The system is designed considering all constraints of a sensor network. It is a real time application and expected to take decision and upgrade its performance in a reactive way.
Index terms - Certainty factor ( CF ) , Electrocardiogram ( ECG ) , knowledge base , leads , learning , rules , self directed learning ( SDL ) , sampling interval ( SI ) ,sensors.
1 INTRODUCTION
———————————— ——————————
ensor nodes can sense, measure, and gather information from the environment and, based on some local decision process, they can transmit the
sensed data to the user. These sensor nodes are equipped with wireless interfaces with which they can communicate with one another to form a network. The design of a WSN depends significantly on the application, and it considers factors like the environment, the application’s design objectives, cost, hardware and system constraints. Sensor networks have a wide variety of important applications [2] , like tracking objects and monitoring processes , patients etc. Clinical deterioration in patients is a major concern for medical institutes. Of these patients, 17% suffer from adverse events such as cardiac or respiratory arrests or other neurological disorder . A retrospective study found that as many as 70% of such events could have been prevented by proper monitoring. A key factor in improving patient outcomes is to detect clinical deterioration early so that clinicians may intervene before a patient's condition worsens. The detection of clinical deterioration is possible because most patients exhibit changes in their vital signs hours prior to an adverse event.

Ayoni Mukherjee is M.Tech student of Computer Science & Engineering at University of Calcutta, India. Email:mukherjee.ayoni@gmail.com
Sanjit Setua is an Associate Professor of Computer Science & Engineering at University of Calcutta, India.
Email : sscomp@caluniv.ac.in
So automatic system aimed at identifying clinical deterioration in patients based on their vital signs is developed. Our system can monitor patients round the clock and regulate its activity , inform health experts accordingly. It is all with static sensor nodes. Though
most of today’s medical application is wired , we opine to use Wireless sensor nodes for this purpose. Our system will learn from its previous decisions and serves the purpose of continuous monitoring. However it is not totally automated, it requires human intervention from time to time. The process will begin with an initial background knowledge and that will be updated in course of time continuously automatically. Health experts can get updated information about the patients by consulting the system whenever necessary. We have also shown performance evaluation.
In section 2 , we present the concept of learning. Section 3 describes Electrocardiogram in brief and
section 4 describes the medical sensor system with an example of cardiac malfunction known as Atrial Flutter .
Section 5 shows performance evaluation and section 6 concludes this paper.
2 LEARNING
A learning theory [4] is an attempt to describe how
people and animals learn, thereby helping us understand the inherently complex process of learning. Learning Theory is rooted in the work of Ivan Pavlov, the famous scientist who discovered and documented the principles governing how animals learn. Learning is commonly defined as a process that brings together cognitive, emotional, and environmental influences and experiences for acquiring, enhancing, or making changes in one's knowledge, skills, values, and world views. Learning as a process focuses on what happens when the learning takes place. Explanations of what happens constitute learning theories. Based upon the controller of objectives and means of learning , we can classify learning into four categories : formal , non formal , informal and self learning.
IJSER © 2011 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 2, Issue 9, September-2011 2
ISSN 2229-5518
A computer program is said to learn from experience ( E
) with respect to some class of task (T) and performance measure ( P ) , if its performance at tasks in T , as
measured by P , improves with experience, E. It is
capable of learning automatically and this is called self- learning, self directed learning ( SDL ) or automated learning. For automated learning , the system must select its own objectives and means. The four key tools for SDL are i) setting goals , ii) planning , iii ) taking actions and iv) self evaluation .
3 ELECTROCARDIOGRAM ( ECG )
The heart normally beats between 60 and 100 times per minute, with many normal variations. This rate is set by
a small collection of specialized heart cells called the sinoatrial (SA) or sinus node. Located in the right
atrium, the sinus node is the heart's natural pacemaker. It has automaticity, meaning it produces electrical discharges all by itself , without the control of the brain.
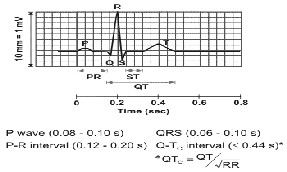
The ECG [1] records the electrical activity that results when the heart muscle cells in the atria and ventricles
contract. It is recorded by a machine called electrocardiograph on a graph paper. The different waves that comprise the ECG represent the sequence of
depolarization and re-polarization of the atria and ventricles. The ECG is recorded at a speed of 25 mm/sec
Electrical activity of the heart is captured by placing electrodes on the skin at different anatomical positions. 10 electrodes provide 12 leads such as I , II ,
III, AvR , AvL, Avf , V1, V2 ,V3, V4, V5 AND V6. ECG displays the voltage between pairs of electrodes. When current flows towards an electrode we get a positive deflection and when it flows away we get a negative deflection. When the current is perpendicular to the lead the deflection is zero or we get an iso-electric line.
Heart rate , Blood pressure, etc). The sensors sense ,
gather information and transmit signals to the mote. The motes are sensor nodes with some processing power and
in them microcontrollers are present in addition to
memory. The mote first digitizes the signals and then give processed ( aggregated, compressed) data to the base station. The number of sensors supported by a mote depends upon the number of ADC channels present in that mote. Both data sampling and wireless transmission are the responsibility of the motes. The processed data is transmitted to the base station from mote either directly or through some relay agents, depending upon the distance of mote from the base station . Health workers access the centralized server with which different base stations use to communicate. So base stations operate in more than one frequency bands for communicating with the server and motes. The system is for monitoring a number of patients at a time in a similar fashion and it is designed to distinguish individual patient’s data. So we can get the benefits of continuous monitoring of critical patients in an automated way with occasional human intervention to take critical decisions. The system is expected to detect any kind of cardiac diseases as quickly as possible and it will provide treatment suggestions accordingly. It also changes sampling interval as required and evaluates own performance periodically with respect to certain predefined parameters and learns from it. System issues an alarm to seek the attention of care-givers for an emergency situation.
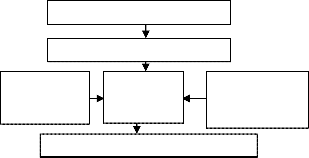
DATA ACQUISITION INTERPRETATION
PATIENT’S
MEDICAL HISTORY
DECISION MAKING
ENGINE
EVIDENCE BASED KNOWLEDGE
BASE
TREATMENT / SUGGESTION
Fig 2. Basic model of medical sensor system
ECG recording for a single heart beat
4 MEDICAL SENSOR SYSTEM
Fig 1.
Centralized server use to take any decision based upon the gathered information by the medical sensors , static patient data such as symptoms , drug habit , test reports etc and a background knowledge . We have represented this background knowledge in the form of
Different medical sensors[3] are attached to the patient’s body at different anatomical positions for sensing different biomedical parameters ( eg: ECG waveform ,
production rules and specified a grammar in BNF form.
As this knowledge base gets updated in course of time , the system performance improves accordingly. In order
IJSER © 2011 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 2, Issue 9, September-2011 3
ISSN 2229-5518
to avoid misdiagnosis , our system suggests for
monitoring any patient at least thrice to arrive at any firm decision and suggest the necessary treatment.
However , the system is intelligent enough to regulate its
sampling interval each time so that the total monitoring time is reduced without compromising the correctness of detection. We have applied certainty factor ( CF ) in each rule , based upon the prior probability distribution of a library of medical cases. Probabilistic abduction is also used for implicit reasoning scheme. The knowledge base is highly ordered to reduce the search time. The knowledge base is divided into different levels for different types of rules. Level-1 rules associate different anatomical positions of body with different ECG leads. Level-2 is for detection of different types of cardiac diseases. Level-3 is to regulate the sampling interval. The level 2 is further sub- divided into a number of zones , one for each disease . A zone is also sub-divided into a number of sub-zones , as required. The rules are organized within a level / zone / sub- zone starting from low CF to high CF. The association between the ECG leads and anatomical positions of sensors are predefined and so for level 1 rules , CF is absolute for all There is no scope of uncertainty in this case. The rules are in antecedent - consequent form. An antecedent of a rule may consist of more than one clauses connected by AND / OR connectives. Each clause is in the form of :
< object – attribute – value > triplet. The attributes used here are mainly multi-valued and Boolean. The
rule base is complete , consistent and avoids conflict ,
redundancy as much as possible.
Level- 1 Rules :
i. < patient – anatomical position – 4th left intercostals space >
<ECG senor – lead – V1, CF=absolute>
ii. < patient – anatomical position – 4th right intercostals space >
<ECG senor – lead – V2, CF=absolute>
iii. < patient – anatomical position – 5th right intercostals space >
<ECG senor – lead – V4, CF=absolute>
Atrial Flutter- A Cardiac malfunction :
Atrial flutter occurs when the atria are stimulated to contract at 200-350 beats per minute usually because
electrical impulses are traveling in a circular fashion around and around the atria. Often the impulses are traveling around an obstacle like the mitral valve,
tricuspid valve or the openings of the superior or inferior
vena cavae. The atrial flutter waves, known as F waves, are observed. F waves are larger than normal P waves
and they have a saw-toothed waveform. Not every atrial
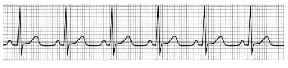
flutter wave results in a QRS complex (ventricular depolarization) because the AV node acts as a filter. Some flutter waves reach the AV node when it is refractory and thus are not propagated to the ventricles. The ventricular rate is usually regular but slower than the atrial rate. A whole number fixed ratio of flutter waves to QRS complexes can be observed, for instance 2:1, 3:1 or 4:1. It is generally detected at leads V1 , V2 , I , II and AvL leads.

Fig 3. ECG waveform for normal sinus rhythm
Fig 4. ECG waveform for Atrial Flutter
Level-2 Rules :
i. < patient – disease – arrhythmia > ^
< ECG waveform – nature – regular saw-tooth
> ^
< ECG waveform – wave - F wave > ^
< ECG waveform– wave – No PR segment >
< patient – disease – Atrial Flutter , CF=
low >
ii. < patient – disease – Atrial Flutter > ^ < ECG
sensor– lead – I >
< patient – disease – Atrial Flutter , CF=
high >
iii. < patient – disease – Atrial Flutter > ^ < ECG
sensor– lead – II >
< patient – disease – Atrial Flutter , CF=
high >
iv. < patient – disease – Atrial Flutter > ^ < ECG
sensor– lead –AvL >
< patient – disease – Atrial Flutter , CF=
high >
IJSER © 2011 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 2, Issue 9, September-2011 4
ISSN 2229-5518
v. < patient – disease – Atrial Flutter > ^ < ECG
sensor– lead – V1 >
< patient – disease – Atrial Flutter , CF=
high >
vi. < patient – disease – Atrial Flutter > ^ < ECG
sensor– lead –V2 >
< patient – disease – Atrial Flutter , CF=
high >
Here a zone within level 2 is shown. As for all patients the abnormality may not be detected at all the
mentioned leads , the rule set for this zone is so formed.
Level-3 Rules : The initial sampling interval ( SI ) is 12
seconds for ECG recording. A small square in the graph paper measures 1 x 1 mm and a large square measures 5 5 mm .In other words, ECG paper has a grid with thick lines 5 mm apart and thin lines 1 mm . On the X axis time is plotted and voltage is plotted on Y axis. Hence one big square is 0.2 sec and one small square is 0.04 sec. On Y axis, one big square corresponds to 0.5 milli volts.
Number of leads = 12
Recording speed = 25 mm/second.
1 small square = 1mm = 0.04 sec ( X-axis ) Number of small squares ( 1 mm ) per lead
= 1/0.04 = 25
Sampling duration ( per lead ) = 1 sec
Total SI = ( 121 ) sec = 12 sec
Total small squares = 12 25 = 300
We have chosen 4 SI s as : 8 sec , 12 sec , 16 sec and
20 sec. Our system compares the result of successive monitoring. If they are exactly alike at all leads , then
we increase the SI to next higher interval , else we decrease SI to next lower interval until the limits at
any end is reached. If result does not match then there is an indication of misdiagnosis or irregularity in cardiac activity and our target is to detect that at its
earliest and inform the care givers accordingly . Some zones of level 3 rules are shown below :
Zone 1 :
<ECGsensor- SI-initial >
<ECGsensor – SI – 12s>
Zone 2 :
<ECGsensor- SI-next higher > :
<ECGsensor – SI – 8s>
<ECGsensor – SI – 12s>
<ECGsensor – SI – 12s>
<ECGsensor – SI – 16s>
<ECGsensor – SI – 16s>
<ECGsensor – SI – 20s>
<ECGsensor – SI – 20s>
<ECGsensor – SI – 20s>
Zone 3:
<ECGsensor- SI-next lower > :
<ECGsensor – SI – 20s>
<ECGsensor – SI – 16s>
<ECGsensor – SI – 16s>
<ECGsensor – SI – 12s>
<ECGsensor – SI – 12s>
<ECGsensor – SI – 8s >
<ECGsensor – SI – 8s>
<ECGsensor – SI – 8s >
5 PERFORMANCE EVALUATION
Performance of any software system is measured
generally in terms of efficiency , productivity , responsiveness and effectiveness. In our system , expected output is nothing but correct diagnosis and treatment ( if any ) .However , the actual output may be correct diagnosis or incorrect diagnosis. Fatal cases denote death of the patients. Inappropriate treatments are those in which the condition of patient deteriorates further than that during admission. We use the following output indicators for performance evaluation :
i. (number of correct diagnosis/ total number of
diagnosis ) 100 %
ii. (number of fatal cases / total number of incorrect diagnosis ) 100 %
iii. (number of inappropriate treatments / total number of treatments ) / diagnosis
iv. Total time from beginning of SI to providing the
result ( diagnosis ) / SI
6 CONCLUSION
The developed system is capable of learning
automatically. After each rule triggering, the patient history is updated with the conclusion of that rule. We
have also kept provision for updating the dynamic
knowledge base. The performance improvement with experience is also a part of self learning . Any traditional rule based expert system can’t learn and lacks
IJSER © 2011 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 2, Issue 9, September-2011 5
ISSN 2229-5518
performance evaluation and treatment. An expert system
asks users questions to arrive at any decision but the most interesting part of our system is that it uses it’s
implicit reasoning scheme to arrive at any decision .
ECG is generally a manual process and can’t provide any treatment suggestion. Instruments like pacemaker / implantable cardio-verter defibrillator (ICD) provides required pacing and shocks but suffers from limitations of lead failure , battery depletion. Lead failure may even require cardiac surgery in some cases. ICD can sometimes provide inappropriate shocks and that is very painful for any patient. Our system uses external , non implantable sensors and also suggests for necessary treatments, as applicable along with the detection of different types of cardiac diseases It thus integrates the benefits of different sensing cardiac instruments.
7 REFERENCES
[1] Zhong Hua , Kanade Takeo , Schwartzman David :
“Sensor Guided Ablation Procedure of Left Atrial
Endocardium “ , MICCAI 2005, LNCS 3750, pp. 1–8,
2005,Springer-Verlag Berlin Heidelberg 2005.
[2] Yick Jennifer, Mukherjee Biswanath, Ghosal Dipak:“Wireless sensor network survey “,Computer Networks 52 (2008) 2292–2330(science direct) ,2008.
[3] Chipara Octav , Lu Chenyang , Bailey C Thomas , Roman Catalin Gruia : “Reliable Patient Monitoring: A
Clinical Study in a Step-down Hospital Unit”
Washington university , 2009-82.
[4] Dunn Lee : “ Theories of Learning “ , first published
on 2000 on OCSLD website , http://www.brookes.ac.uk/services/ocsld/resources/briefi
ng_papers/learning_theories.pdf.
IJSER © 2011 http://www.ijser.org