Inte rnatio nal Jo urnal o f Sc ie ntific & Eng inee ring Re se arc h, Vo lume 3, Issue 3, Marc h-2012 1
ISS N 2229-5518
Squamous cell carcinoma of the vulva in a virgin patient with Turner syndrome
Soniya priyadharishni.A.K, Dr.M.Sridhar, Dr.M.Rajani
Abs tract— Tw o types of gynecologic tumors are commonly described in the Turner syndrome, the f irst one is gonadoblastoma, w hich occurs in patients w ith Y chromosome abnormalities, and the second one is endometrial carcinoma w hich is mostly related w ith exogenous estrogen usage. Here, w e describe an extremely rare case of squamous cell carcinoma of the vulva in a virgin w oman w ith Turner syndrome. A 35-years old single, virgin w oman ref erred to our Oncology Department w ith w arty, necrotized, exophytic 6-7 cm vulvar mass. She had a history of primary amenorrhea and mosaic Turner syndrome w as determined in her karyotype analysis. Biopsy specimen of the vulvar mass revealed squamous cell carcinoma of the vulva, and total vul- vectomy w ith inguinal f emoral lymphadenectomy w as perf ormed. The postoperative course w as uneventf ul and there has been no recurrence of the disease up to date. Women w ith Turner syndrome have streak ovaries that produce very low estrogen and the squamous cell carci noma of the vulva may have developed at an early age w ith Turner syndrome because of this low estrogen value similar to postmenopausal w omen. The current case is a special case due to its age of occurrence, virgin and Turner syndrome status.
Inde x Terms— Exophytic, Karyotype, Lymphadenectomy, Turner syndrome, vulvar.
—————————— ——————————
1 INTRODUCTION
Turner syndrome (TS) is the most common chromosomal a b- normality in females, affecting 1:2,500 live female births, and is a condition involving total or partial absence of one X chro- mosome in all or part of the cells, reduced final height, a b- sence of female sex hormones, and in most cases infertility. Some cancer types, such as colon cancer, thyroid carcinoma, and acute myeloid leukemia were reported in patients with TS. Two types of gynecologic tumors are commonly described in TS, the first one is gonadoblastoma, which occurs in pa- tients with Y chromosome abnormalities, and the second one is endometrial carcinoma which is mostly related with ex- ogenous estrogen usage. Here, we describe an extremely rare case of squamous cell carcinoma of the vulva (SCCV) in a young virgin woman with Turner syndrome.
2 C ASE REPORT
A 35-years old single, virgin woman referred to our Oncology Department with wart like, necrotized, exophytic vulvar mass. The size of the lesion was around 6 -7 cm. It was originated from the left labia majora and extended to the clitoris and urethral meatus. There was a suspicious palpable right groin lymph node. Biopsy specimen of the vulvar mass revealed SCCV (well- differentiated).
———— ——— ——— ——— ———
Soniyapriyadharishni.A.K. is currently pursuing Ph.D program in Bioinfor- maticts in Bharath University, India,
Dr.M.Sridhar,D.Sc.,A.Sc., is currently the Director A&P inBharath Universi-
ty, India
Dr.M.Rajani,D.Sc.,is currently the Director R&D in Bharath University,
India.
She had a history of primary amenorrhea, and the clinical di- agnosis of TS before but she did not have the medical reports proving TS. Therefore, karyotype analysis was performed in our hospital's Genetic Department by the conventional G-banding method using peripheral blood lymphocytes. Mo- saic TS was determined in her karyotype analysis. According to her history, she had no sexual relationship of any kind. She had received estrogen replacement therapy for only 6 months, and she had no history of toba cco use. Her family history was unremarkable. The serum hormonal assay revealed, FSH,
64.86 mIU/mL; LH, 38.45 mIU/mL; progesterone, 0.38
pg/mL; and estradiol, 14.54 pg/mL, all of the other laboratory
results were normal.
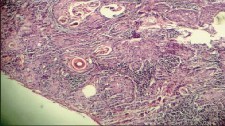
Total vulvectomy with inguinal femoral lymphadenectomy was performed. The final histological diagnosis was SCCV (Fig. 1), and vascular or neuronal invasion was not observed. The su r- gical margins were free of disease. The inguinal and femoral lymph nodes were negative. The clinicopathologic stage (FIGO) was stage II. The postoperative course was uneventful and there has been no recurrence of the disease up to date.
Fig. 1-Microscopic f inding of the patient; squamous cell carcinoma of the vulva, tumoral cell groups inf iltrate the stroma irregularly (H&E, ×100).
IJSER © 2012
http :// www.ijser.org
Inte rnatio nal Jo urnal o f Sc ie ntific & Eng inee ring Re se arc h, Vo lume 3, Issue 3, Marc h-2012 2
ISS N 2229-5518
4 DISCUSSION
Cancer of the vulva which is primarily a disease of postmen o- pausal women, with a peak incidence in the late 60's is respon- sible for approximately 3-5% of gynecologic cancers. SCCV is the most common type among the vulvar cancers. This disease typically develops in older women (in their seventh or eighth decade of life) and is rarely seen in women younger than 35 years of age. The current case is a special case due to its age of occurrence, virgin and TS status. To our knowledge, there are no published reports of SCCV in a young virgin woman with TS.
The etiology of SCCV is not well known and epidemiological evidence to date suggests that th ere are two etiologic path- ways responsible in carcinogenesis. The first one is often seen in older women and related with non -neoplastic epithelial disorders, mainly atrophic dystrophy which is seen in low estrogen states. The second one is often seen in younger wom- en and is associated with human papillomavirus (HPV) infec- tion. The study performed by Jones et al. suggested an increas- ing incidence of vulvar intraepithelial neoplasm related with HPV in women younger than 50 years of age. Another study reported by Huang et al. showed the importance of HPV inte- gration in both cervical and vulvar cancers. However; both of the etiologic paths were not appropriate for explaining the mechanism of the disease in our young and virgin case. Other risk factors include current tobacco use, the presence of genital warts, and multiple sexual partners, but these were also not present in our case.
In the English literature, we found only one case that pre- sented with vulvar carcinoma in a TS patient. In this report Iwamoto et al. concluded that the vulvar carcinoma may be related with low estrogen levels in TS like in elderly postme- nopausal women. In our opinion this etiologic path may ex- plain our cases' condition.
In conclusion, women with TS have streak ovaries that pro- duce very low estrogen and SCCV may have developed at an early age with TS because of this low estrogen value similar to postmenopausal women. Here, we described the first case of SCCV in a young virgin patient with TS.
5 FOOTNOTES
No potential conflict of interest relevant to this article was re- ported.
6 R EFERENCES
[1] Elsheikh M, Dunger DB, Conway GS, Wass JA. Turner's syndrome in adult- hood. Endocr Rev. 2002;23:120–140.
[2] Chaganti RS, Bailey RB, Jhanwar SC, Arlin ZA, Clarkson BD. Chronic myelo- genous leukemia in the monosomic cell line of a fertile Turner syndrome mosaic (45,X/46,XX) Cancer Genet Cytogenet. 1982;5:215–221.
[3] Cabanas P, Garcia-Caballero T, Barreiro J, Castro-Feijoo L, Gallego R, Arevalo T, et al. Papillary thyroid carcinoma after recombinant GH therapy for Turner syn- drome. EurJ Endocrinol. 2005;153:499–502.
[4] Sybert VP, McCauley E. Turner's syndrome. N Engl J Med. 2004;351:1227–1238.] [5] Gadducci A, Cionini L, Romanini A, Fanucchi A, Genazzani AR. Old and new
perspectives in the management of high-risk, locally advanced or recurrent, and
metastatic vulvarcancer. Crit Rev Oncol Hematol. 2006;60:227–241.
[6] Madeleine MM, Daling JR, Carter JJ, Wipf GC, Schwartz SM, McKnight B, et al. Cofactors with human papillomavirus in a population-based study of vulvar can- cer. J Natl CancerInst. 1997;89:1516–1523.
[7] CanavanTP, CohenD. Vulvarcancer. Am Fam Physician. 2002;66:1269–1274.
[8] Stroup AM, Harlan LC, Trimble EL. Demographic, clinical, and treatment trends among women diagnosed with vulvar cancer in the United States. Gynecol Oncol.
2008;108:577–583.
[9] Jones RW, Baranyai J, Stables S. Trends in squamous cell carcinoma of the vulva:
the influence of vulvarintraepithelial neoplasia. Obstet Gynecol. 1997;90:448–452.
[10] Huang FY, Kwok YK, Lau ET, Tang MH, Ng TY, Ngan HY. Genetic abnormal- ities and HPV status in cervical and vulvar squamous cell carcinomas. Cancer Ge- net Cytogenet. 2005;157:42–48.
IJSER © 2012
http :// www.ijser.org