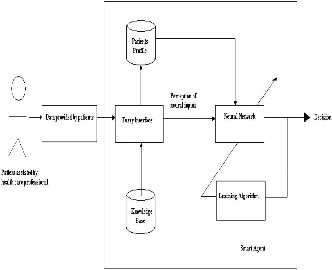
Fig. 1 shows the functional architecture of the fuzzy neural smart agent based medical diagnostic system
International Journal of Scientific & Engineering Research Volume 4, Issue3, March-2013 1
ISSN 2229-5518
FPGA Based Critical Patient Health Monitoring Using
Fuzzy Neural Network
Dipali L.Gaikwad #1, Prabha Kasliwal#2
#Electronic Department, Pune University
MIT Academy Of Engineering Alandi, Pune, India. dipaligaikwad11@gmail.com prabha.kasliwal@gmail.com
Abstract—
Keywords— Medical diagnosis, Fuzzy neural network. Field programmable gate array Critical condition
Medical diagnosis is a complicated and judgmental process, based not only on medical knowledge derived from books and literatures and
data obtained from various pathological
tests, but also depends largely on experience, judgment and reasoning which essentially are the functions of human brain .However, diagnostic decisions made by physicians are arbitrary and highly variable (within one physician and between physicians) and often lacking explanation or rationalization.
However, in third world countries like India, doctors are scarcely available in rural areas. A recent statistical data shows that 75% of qualified consulting doctors reside in urban areas and another
23% in semi-urban areas, and only about 2% of
doctors reside in rural areas, where, unfortunately, nearly 78% of Indians reside .This has created an unwarranted imbalance in patient-doctor ratio of more than 10,000 patients for one doctor in rural India. Apart from the acute scarcity of physicians, lack of availability of electricity is quite common in rural areas of third world countries like India. Such prosaic problems necessitate the use of an inexpensive, portable, low power battery operated high-speed. equipment that can have the intelligence to predict an imminent health hazard and red alert the patients in rural sectors to contact the doctors for necessary care.
Advantage of patient profiling and storage of sets of data in non-volatile memory of the instrument, is an additional advantage in rural areas of third world
IJSER © 2013 http ://www.ijser.org
International Journal of Scientific & Engineering Research Volume 4, Issue3, March-2013 2
ISSN 2229-5518
countries where archiving of medical records is poor, and in industrialized countries, where physically and mentally in capacitated older generations cannot maintain records. The notion of an instrument for first order clinical diagnoses of chronic cases in particular, becomes important when patients and doctors are physically apart from each other and doctor needs to remain vigilant about early signal of deterioration of health of patients
However, in the backdrop of scarcity of physicians especially in the rural areas, an instrument with some auto-decision making support can be used for early diagnosis of problems related to specified systems of patients’ bodies. These systems can aid the physicians or the health care professionals in absence of the physicians to predict the pathophysiological state of a patient knowing the past pathophysiological data and red alert the physician or the health care professionals in case a critical condition of the patient occurs so that the health care professionals can communicate with the physician at the remote location in time and the physicians at the remote referral centres can provide medical ailments to the patient.
Fig. 1 shows the functional architecture of the fuzzy neural smart agent based medical diagnostic system. At least two entities, viz. patient and smart agent are required in this concept of smart agent based diagnostic system. The patients are the providers of data under the assistance of health care professionals who need not be physicians. The smart agent is represented by a weakly coupled fuzzy neural system that can predict the future pathophysiological state of a patient in presence of past pathophysiological data. The weakly coupled fuzzy neural network is basically a two unit composite system comprising of a fuzzy system placed before a neural network. The fuzzy interface makes an approximate inference about the current
state of the patient from the current patient data being entered into the smart agent. The membership values obtained from the output of the fuzzy interface are supplied to the input of the neural network for making a decision regarding the future pathophysiological state of the patient.
.
Fig. 1 shows the functional architecture of the fuzzy neural smart agent based medical diagnostic system
The fuzzy interface discussed in Section 2 performs fuzzifica- tion of patient data. The data from the patient such as height or weight data cannot always be trusted as they are subjected to the quality and accuracy of measuring units and the skill of the technician. Moreover, based on a single data, it would be highly uncertain to make an accurate decision about the future physiological state of the patient. So the patient data have been fuzzified with the objective of transformation of periodic measures into likelihoods that the
1.Body mass index,
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 4, Issue3, March-2013 3
ISSN 2229-5518
2 Blood glucose,
3.Creatinine,
4.Systolic blood pressure
5. Diastolic blood pressure .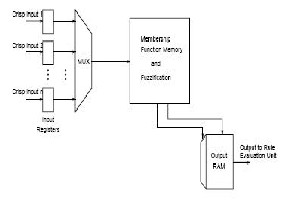
. Fig 2 .Fuzzificationu unit
The architecture of the fuzzy neural network is shown in Fig. 3. The left most layer is the input layer, which accepts the membership function values, which are presented to the hidden layer. The in put layer consists of 60neurons,the hidden layer consists of 18 neuron and the output layer consists of three neurons. The neural network calculates the possibilities of the pathophysiological parameters to below, moderate or high at the next instant of time .The connection between the input layer and the hidden layer is shown as interconnection network box for clarity. There is a connection between every neuron in the input layer and every neuron in the hidden layer .The weighted sum of the possibility values from the hidden to the output layer indicates the criticality of the current condition of the patient which is indicated as an output to the neural network .The inputs are presented to the input layer in the form of a 60 tuple(b(1), b(2),……..b(10), g(1), g(2),……,g(10), c(1), c(2),…….,c(10), u(1), u(2),……..,u(10), s(1),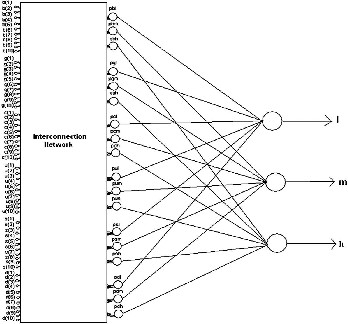
s(2),…….,s(10), d(1), d(2),…….,d(10)). Initially only b(1), g(1), c(1), u(1), s(1) and d(1)have non- zero values, while others have zero values. At the next instant of time(after10 days), when a new set of data is entered, b(2), g(2), c(2), u(2), s(2) and d(2) are updated to non-zero values and soon. As new sets of data are entered ,the old sets of data are up dated .Thus after 10 sets of data collected at 10 days interval are entered ,when the 11th set of data are entered ,the new set of data goes to b(10), g(10), c(10), u(10), s(10) and d(10) and b(9), g(9), c(9), u(9), s(9) and d(9) are up dated with the previous values of b(10), g(10), c(10), u(10), s(10) and d(10), respectively, and so on.
Fig. 3 The architecture of the fuzzy neural network
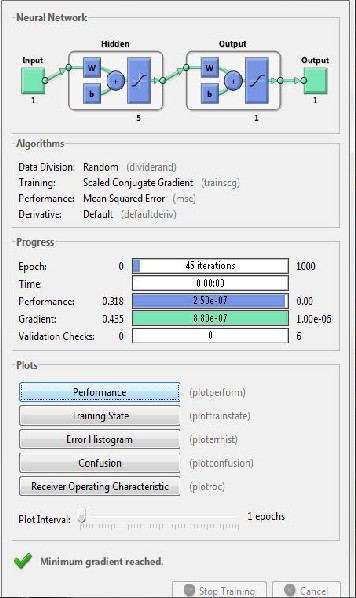
The fuzzy neural network has been implemented on an FPGA. The proposed system has been implemented on an Altera Cyclone family EP1C6Q240C8 FPGA chip. The proposed system could have also been implemented using software. Yet, the main disadvan- tage of the software solution is that a powerful computer is to be used to
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 4, Issue3, March-2013 4
ISSN 2229-5518
run the software for achieving reasonable speed and accuracy.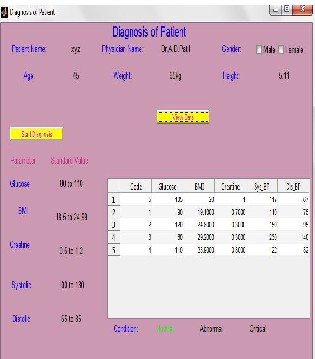
This could be an actual drawback of the software approach, only if even more complex systems that could probably cover many different infected parts of the human body are to be constructed. The main reason for a hardware based implementation is the need for an inexpensive portable diagnostic system. The main disadvantage of an ASIC based hardware is the high development cost and the low configurabilit y it allows for. The FPGA solution ensures that new changes in the proposed diagnostic algorithm can be mapped onto the hardware without having to make costly changes
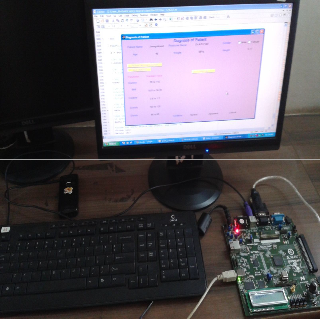
Fig 5. Picture on the system on board
IV CONCLUSIONS
The current work focuses on the application of neuro-fuzzy synergism to detect at an early stage the probable approaching critical condition of a patient. It explains the usage of fuzzy neural networks in medical diagnosis systems and the extended example on the problem of earl y detection of approaching critical renal condition of patients. In order to improve the accuracy of diagnosis, optimal synaptic weights have been found out using the inverse delayed function model of the neuron.
Fig4. graphical user interface
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research Volume 4, Issue3, March-2013 5
ISSN 2229-5518
pressures are considered as pathophysiological parameters. The fuzzy neural network has been suitably trained and tested with real patient data to find out the correspondence with the decision being given by the fuzzy neural network and the actual pathophysiological state of the patient.
1) M. Kukar, Transductive reliability estimation in medical diagnosis, Artificial Intelligence in Medicine 29 (2003) 81–106.
2) D.M. Eddy, The challenge, Journal of
American Medical Association 263 (1990)
287–290.
3) R.J. Lilford, S.G. Pauker, D.A. Braunholz, J.
Chard, Decision analysis and the implementation of research findings, Biomedical Journal 317 (7155) (1998) 405–
409.
Fig. 6. Neural network training process result.
The neurons that are considered in the proposed network are devoid of self connections unlike the previously proposed networks based on inverse delayed function model of neurons where self-connected neurons have been assumed. For diagnosis purposes, body mass index (B.M.I.), glucose, creatinine, systolic and diastolic blood
4) S. Zhang, H. Hu, H. Zhou, An interactive internet based system for tracking upper limb motion in home based rehabilitation, Medical and Biological Engineering and Computing 46 (3) (2008) 241–249.
6) K.Y.C. Goh, C.K. Lam, W.S. Poon, The impact of teleradiology on the inter- hospital transfer of neurosurgical patients, British Journal of Neurosurgery 11 (1997) 52–56.
7) J.F. Heautot, B. Gibaud, B. Catroux, P.H.
Thoreux, E. Cordonnier, J.M. Scarabin, Influence of the teleradiology technology (N-ISDN and ATM) on the inter- hospital management of neurosurgical patients, Medical Informatics 24 (1999) 121–134.
8) D. Hailey, P. Jacobs, Assessment of
Telehealth Applications, Alberta Heritage Foundation for Medical Research, Edmonton (Alta), 1997.
IJSER © 2013 http://www.ijser.org