Inte rnatio nal Jo urnal o f Sc ie ntific & Eng inee ring Re se arc h, Vo lume 3, Issue 3, Marc h-2012 1
ISS N 2229-5518
ECG signal analysis used as confirmative tool in quick diagnosis of Myocardial Infarction
Manjusha Joshi, Dr. K.D.Desai
—————————— ——————————
1 INTRODUCTION
ardiovas cular diseas e is the world's leading killer, account- ing for 16.7 million or 29.2 per cent of total global deaths in 2003. The World Health Organization (WHO) estimates
that 60 per cent of the world's cardiac patients will be Indian by
2010. Als o it has been found out that India has more number of cardiovascular deaths claiming younger population than in America [1]. The major reasons contributing to sudden deaths are due to myocardial infarction (commonly known as heart attack). Apart from deaths due to accidents myocardial infarc- tion is the most commonly found ep isode in sudden cas ualty. The time from the ons et of myocardial infarction to the trea t- ment for the s ame is very crucial. Therefore it is very essential that diagnos is of the clinical symptoms should be as fast as poss ible. The onset of my ocardial infarction results in to the changes in ECG of the p atient. Thes e changes can be used as tools of diagnos is . Before the phys ician is available the para- medical s taff can start the preparatory treatment if the myocardi- al infarction is confirmed. Such quick confirmation is poss ible by us ing s ignal process ing techniques applied to a normal ECG and the ECG of the patient under diagnos is . The propos ed paper discusses the confirmatory changes in ECG in case of different types of myocardial infarction and co mpares the patient’s ECG with normal ECG. The ECG images available are converted in to s ignal s o that the s ignal process ing tools can be applied to it. The s ignal process ing tool of cross correlation and auto correla- tion can confirmatively ass ess the degree of s imilar i- ty/diss imilarity between the two s ignals .[2] This information can be us ed by the paramedical staff to ass ess whether the patient is suffering from myocardial infarction or a casual ang ina.Also the poss ibility of ectopic beats which can be fals ely cons idered as a cas e of arrhythmia can be ruled out by the following test.
———— ——— ——— ——— ———
Manjusha Joshi is currently pursuing Ph.D. program in biomedical eng i- neering NMIMS(deemed to be) University, India, PH -919619102215-.
Dr. K.D.Desai is Director K.C.College, Mumbai University, India, PH-
919967002026. E-mail:kddesai@hotmail.com
)
The propos ed paper us es the ECG of the patient and the normal ECG of the patient if available before onset of the diseas e. [3] If the normal ECG of the s ame p atient is not available, then any other normal ECG can be us ed for tool for co mparis on.
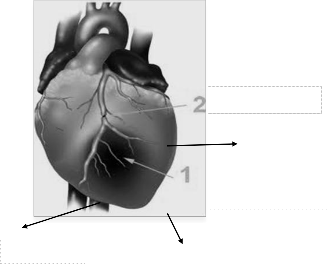
Myocardial Infarction refers to damage or death (infarction) of heart mus cle (myocardium). The damage results from the inte r- ruption of blood s upply to part of the heart caus ing heart cells to die. This is most commonly due to occlus io n (blockage) of a coronary artery following the rupture of a vulnerable atheros cle- rotic plaque, which is an uns table collection of lipids (choles ter- ol and fatty acids ) and white blood cells in the wall of an artery. If left untreated for a sufficient period of time this leads to per- manent death of heart wall mus cle. Since heart wall expans ion and contraction is essential for proper functioning of heart, the damage of the wall affects the functioning of the heart res ulting into heart failure. The type of infarction depends upon which part of the heart wall is damaged. The heart wall is mainly d i- vided in three zones as shown in figure-1.
The prominent types of infarction are –
1. Anterior infarction
2. Pos terior infarction
3. Inferior infarction
ECG is non invas ive, safe tool t hat gives ins tantaneous res ults . The ECG of an infracted heart is different than that of a normal heart. The change in ECG is the dependent upon the location of infarct.[4]
The anterior wall infarction can be properly repres ented by AVL
and V5-V6 leads . (Refer figure 2a)
The inferior myocardial infarction will be properly represented by AVF and V2-V3 leads . (Refer figure 2b)
IJSER © 201 2
Inte rnatio nal Jo urnal o f Sc ie ntific & Eng inee ring Re se arc h, Vo lume 3, Issue 3, Marc h-2012 2
ISS N 2229-5518
Blocked art ery
P ostrior wal l
Infract ed zone
Figure 2b Required ECG leads repres enting Inferior Infarction
Ant erior wall
Figure-1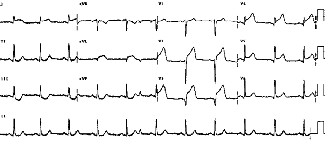
Inferior wall
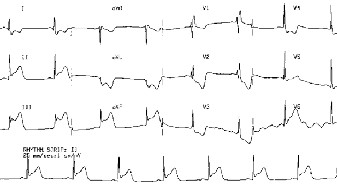
The posterior infarction is not clearly vis ible in the ECG. Over all changes in ST s egment can be the confirmative indication. These changes in the ECG can be compared to that with the normal ECG. (Refer figure 2c).
The ECG is obs erved to be changing depending upon the dura- tion of the infarct. By and large the confirmatory change in ECG is the ST segment depress ion and tall T wave with s ymmetrical taper.
The corresponding ECGs are as s hown in the figure.2 [5]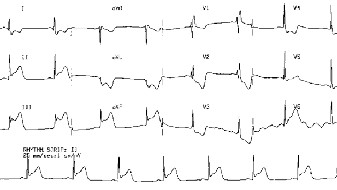
Figure 2a ECG of Posterior Infarction.
Figure 2c Required ECG leads rep resenting Anterior Infarction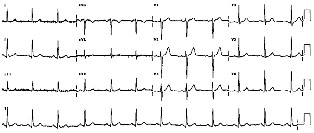
Figure 2c Normal ECG
Bio s ignals are highly subjective. Though there are some s ta n- dard parameters of the ECG s ignals , the parameters tend to vary from pers on to person time to time. So it is not poss ible to build confirmative heuris tic diagnostic algorithm to detect the abno r- mality. The s uitable tool for the confirmative diagnos is is by us ing the cross correlation of the no rmal and abnormal s ignal. The accuracy of the diagnos is can be achieved by cross correlat- ing the two s ignals over s ufficiently long duration.
ECG Images of normal and different types of infraction are us ed from s tandard MIT-BIH databas e. The duration of s ignals us ed is for 120 s ec. which is s ufficiently large to ensure accuracy of results .
It is essential to convert the images to s ignals to as certain the
accuracy of the result. [5] This can be done by the implementing gray level s licing and then boundary extraction algorithm. The
IJSER © 201 2
Inte rnatio nal Jo urnal o f Sc ie ntific & Eng inee ring Re se arc h, Vo lume 3, Issue 3, Marc h-2012 3
ISS N 2229-5518
extracted boundary can be us ed as s ignal fit to us e for applying further cross correlation and auto correlation techniques . [6]
The res ulting summation values for autocorrelation and cross correlation can be us ed as confirmative parameters to diagnos e the dis ease.
It is evident from table-1and als o graph-1 that the cross correla- tion values are at least half that of the autocorrelation. It a co n- firmative pos itive diagnos tic indication that proves the ECG change are prevalent over a s ufficiently long period of time.
Also the autocorrelation values are found to be higher for the
diseas e that is 15 days old compared to that if the dis eas e is s ix months old. This proves the fact that longer the duration of myocardial infarction wors e will be the s ituation.
It has also been evident from the table that values of anterior
infarction are much higher than the other dis eas es . This is purely incidental as we have taken the specimen of one patient.
Table 1
More work can be done by taking more s amples and results and discuss ion can be further more confirmative. Also it is poss ible Also it is poss ible to explore more by taking different time in- terval windows of myocardial infarction. More work is als o poss ible if one takes ECGs specific to one dis eas e and actual patient data.
7 References
[1]― cardiovascular disease t rends in India‖
www.expresshealthcaremgmt.com/20041215/crit icare06.shtml.
[2]‖Digit al Signal Processing Principles, Algorit hms and Applicat ions‖
Fourth Edit ion John G. Proakis and Dimitris G. Manolakis.
[3] ― Risk of Acut e Myocardial Infarct ion, St roke, Heart Failure, and Death in Elderly Medicare Pat ient s Treated With Rosiglit azone or P ioglitazone‖, David J. Graham, MD, MPH, Rita Ouellet -Hellst rom, PhD,Thomas E. Ma-
Curdy, PhD.
[4]‖A system for the detect ion of diabet ic myocardial infarct ion ―
K.D.Desai PHD Thesis, university of Mumbai, February 1996. [5]www.ECGDATA.com st andard ECG database.
[6]‖ Image Processing Using MATLAB Codes‖ ,second edit ion. By
Dhananjay K. Theckedat .
IJSER © 201 2