Fertility is highest in Northern Nigeria, where women have an average of almost 7 children in their lifetime. The survey results show fertility in Nigeria has remained at a high level over the last 17 years with 6 births per woman.
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1068
ISSN 2229-5518
CASE STUDY: NIGERIA DEMOGRAPHIC AND HEALTH SURVEY, 2003 &2008
Authors: O. B. Aladeniyi , A. H. Bello, P.O.OLOPHA and O.O ALABI
Department of Mathematical Sciences, Federal University of Technology, Akure. Nigeria.
The study is on the Demographic analysis on proximate and contextual determinant of fertility in Nigeria. It employs the use of secondary source of data from Nigeria Demographic and Health Survey between 2003 – 2008.The aim is to study how proximate and contextual determinant contribute to the reduction of fertility among currently married women in Nigeria. The methodology are the use of Bongaart model for the analysis of proximate determinant of fertility. The percentage, proportion and chi- square were also used in the area of analysis. The results of the analysis shows that contextual determinants can influence fertility only through the proximate determinant. The proportion of married women remains the most important proximate determinant responsible for reduction in
fertility in Nigeria. The analysis revealed that age at first marriage rose from 16.6years to 18.3years,contraceptive used increased from 12.6% to 14.6%.Result of chi-square test shows that contextual determinant is statistically significant in relation to the proximate determinant of fertility.
Keyword: Bongaats Model – TFR=Cm x Cc x Ca x Cs x Ci x TF
TFR: Total Fertility Rate
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1069
ISSN 2229-5518
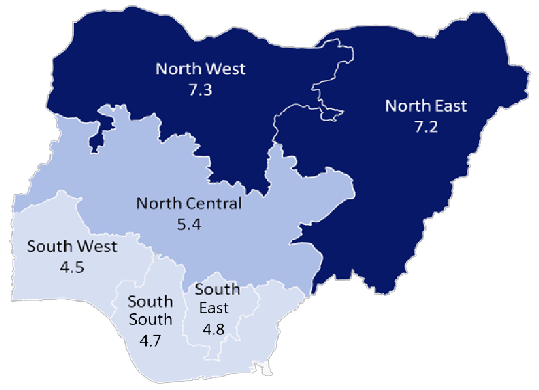
The annual population growth rate in Nigeria is 2.27 (United Nations 2006), the 2006 Population and Housing Census puts Nigeria’s population at 140,431,790, with a national growth rate estimated at 3.2 percent per annum. With this population, Nigeria is the most populous nation in Africa. Nigeria’s population is unevenly distributed across the country. Large areas in the Chad Basin, the middle Niger Valley, the grassland plains, among others, are sparsely populated. The average population density for the country in 2006 was estimated at 150 people per square kilometer. Women in Nigeria have an average of 6 children. The average number of children per woman ranges from 5 in urban areas to 6 in rural areas. Fertility has not changed since the 2003 NDHS. Fertility varies dramatically by zone. Women in the South West zone have an average of 5 children compared with 7 children per women in the North West zone. Fertility also varies with mother’s education and economic status. Women who have more than secondary education have an average of 3 children, while women with no education have 7 children. Fertility increases as household wealth decreases. The poorest women have almost twice as many children as women who live in the wealthiest households (7 versus 4 children per woman). Studies have reported that fertility transition is in progress in most Sub-Saharan African countries (Bongaarts, 2008; Guttmacher, 2008), Nigeria (Feyisetan and Bankole 2002) and Guinea (measuredhs, 2007). Studies and surveys done in some regions and among ethnic groups suggest that fertility is declining in Nigeria (Caldwell et al. 1992). However, these studies and surveys are devoid of national representativeness as they are localized in specific regions or selected ethnic groups. Thus, they cannot be used as a national reference. The trend of the total fertility rate (TFR) from the three consecutive Demographic and Health Surveys in Nigeria did not show any meaningful decrease over time. Based on Demographic and Health Surveys the claim that fertility is decreasing in Nigeria may be misleading, because the
data reported for the past three NDHS surveys are almost the same.
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1070
ISSN 2229-5518
FERTILITY BY ZONES
Fertility is highest in Northern Nigeria, where women have an average of almost 7 children in their lifetime. The survey results show fertility in Nigeria has remained at a high level over the last 17 years with 6 births per woman.
The aim of this study is to identify the fertility reduction contribution of the proximate determinants of fertility among currently married women in Nigeria. The objectives are
• To analyze the proximate determinants of fertility in the 2003 and 2008 NDHS surveys and to identify the fertility reduction contribution of the proximate determinants in order to describe, explore and explain the association between proximate determinants and fertility.
• To describe and investigate the pattern of association between the proximate determinants and indirect or contextual determinants in regard to their socio economic and environmental characteristics among currently married women aged 15 to 49 years.
The study population was based on women of reproductive ages 15-49 in Nigeria, the NDHS covered a population of about 7,620 and 33,385 women in 2003 and 2008 respectively and this population was used for the analysis on trends and fertility reduction contribution. While the study population for the study on
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1071
ISSN 2229-5518
relationship between proximate and contextual determinants was based on currently married women in
Nigeria in 2008, the NDHS covered a population of 23,578 women.
To what extent has the proximate and contextual determinants contributed to reduction in fertility rate in Nigeria? And how can they be improved on to further decrease the fertility rate?
p=.05 (α=95%)
Decisino Rule: Reject H0t (t = 1, 2,…, 10) if P-value ≤ α, otherwise, do not reject.
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1072
ISSN 2229-5518
Nigeria has five records of census data, 1952/53, 1963, 1973, 1991 and 2006. The 1973 census was cancelled because it was confounded with underestimation and overestimation . None of the censuses conducted in Nigeria was devoid of gross allegations of underestimation or overestimation. However, the 2006 census in Nigeria has been considered the most free and fair exercise. Four Nigeria Demographic and Health surveys (NDHS) have been conducted in 1990, 1999, 2003 and 2008. Nigeria also conducted the National Rural Demographic Sample survey in
1965/66 and the Sentinel Survey in 1992-1994. Thus, the estimates of total fertility rate from the world fertility survey (WFS), censuses, post enumeration survey (PES) and DHSs were properly documented. There are many explanations for the discrepancies in the fertility rate observed in different surveys conducted in Nigeria. There is the possibility of distorted fertility rates where different survey coverage periods overlap due to erroneous date of birth records.
Furthermore, there is often a tendency of pushing more recent births back in time, which depletes the rates for the five years before and inflates those of 5 to 9 years and 0 to 14 years before the survey. In addition, births that occurred in the more distant past may be brought forward into periods nearer the survey. Also a number of factors have influence on fertility; whether their effect is indirect or direct. However, a lot of studies and researches on the causes of fertility levels and their differentials had previously been conducted by efforts of measuring the direct impact of socio economic factors on fertility such as median age at marriage (Feyisetan and Bankole, 2002; Harwood-Lejeune, 2001), education (Vavrus and Larsen, 2003), contraception (Westoff and Bankole, 2001), postpartum infecundibilty (Makinwa-Adebusoye and Feyisetan,) and prevalence of polygamy (Feyisetan and Togunde, et al., 1988). There are also studies on aspects of sexual behaviour related to fertility, impact of HIV/AIDS epidemics (Zaba et al. 2004; Ntozi et al. 2001; Lewis et al. 2004), abortion (Diallo, 1996), fertility desire (Bongaart,
1990) and culture and tradition (Isiugo-Abanihe, 1994) until Davis and Blake developed a framework that recognised both indirect and direct determinants of fertility in the mid-1950s (Bongaarts, 1978; Bongaarts, 1982; Stover 1998). Figure 2.1 illustrates the simple sequence of relationships among the determinants of fertility as recognised by Davis and Blake (Bongaarts, 1978; Bongaarts, 2003). To produce a sharper and more holistic understanding on fertility variations, the World Fertility Survey (WFS, 1977) strongly advised that a fertility analysis should cover both indirect and direct determinants.
The proximate determinants of fertility are defined as the biological and behavioural factors through which, and only through which, the indirect variables - social, economic, and environmental variables - affect fertility (Bongaarts,
2003). Most of the Sub Saharan countries began to undergo fertility transition about four decades ago (Bongaarts,
2005). Analysis of the Nigeria Fertility Survey (NFS) 1981-82 shows that first marriage is the main proximate determinant of fertility, followed by breastfeeding and postpartum sexual abstinence (Chimere 1990a). Chimere (1990a) observed that breast-feeding and post-partum abstinence curbed childbearing in the rural areas substantially more than in urban areas. However, the examination of proximate variables on urban and rural fertility did not show
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1073
ISSN 2229-5518
reasonable differences. Fertility transition suggests that there has been a shift from the variables driving high fertility rates to low fertility levels. A proximate determinant is distinguished from other determinants of fertility by its primary characteristic: its direct effect on fertility. Other variables which were identified as indirect variables (socioeconomic, cultural, and environmental) could only affect fertility through these intermediate variables. Marriage and the onset of permanent sterility specifically determine the duration a woman’s reproductive period will last. Other proximate determinants that influence the rate of childbearing and the duration of birth intervals are contraceptives, age at sexual intercourse, postpartum amenorrhoea, abstinence, frequency of sexual activity and induced abortion (Kaida et al. 2006).
Based on the analysis of the three NDHSs carried out by Ibisomi (2008), post-partum in fecundibility had the greatest inhibiting effect on fertility followed by marriage/sexual activity, contraception and then sterility, Bongaarts model showed that these proximate indices collectively reduced total fecundity by 12.5, 8.9 and 9.5 births in the total sample of married women in 1990, 1999 and 2003 respectively (Ibisomi, 2008)
Davis and Blake (1956) developed a framework in order to describe the intermediate variables of fertility. It covered three stages of human reproduction, specifically, intercourse, conception and gestation. These stages were then divided into 11 factors which would directly affect the level of fertility. They classified these eleven variables into three groups, as shown in table 2.1 below.
a. Factors affecting exposure to intercourse (Intercourse Variables)
• The formation and dissolution of (sexual) unions during the reproductive period:
1. Age of entry into a sexual union
2. Permanent celibacy: proportion of women never entering into a sexual union)
3. Amount of reproductive period spent after or between unions: i). When unions are broken by divorce, separation, or desertion ii). When unions are broken by death of husband
• The exposure to intercourse within unions:
1. Voluntary abstinence
2. Involuntary abstinence (from impotence, illnesses, unavoidable but temporary separations)
3. Coital frequency (excluding periods of abstinence)
b). Factors affecting exposure to conception (Conception Variables)
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1074
ISSN 2229-5518
1. Fecundity or infecundity, as affected by involuntary causes
2. Use or non‐use of contraception
3. Fecundity or infecundity, as affected by voluntary causes (sterilization, sub‐incision, medical treatment).
c). Factors affecting gestation and successful delivery (Gestation Variables)
1. Foetal mortality from involuntary causes
2. Foetal mortality from voluntary causes
Despite Davis and Blake’s pioneering work, it had proved difficult to quantify the relationships between the intermediate fertility variables and fertility to produce a simple reproductive model (Bongaarts, 1978; Lucas, 1994). This had gone on for almost two decades until Bongaarts (1978) developed a framework for analysing the proximate determinants of fertility. He used those 11 intermediate fertility variables proposed by Davis and Blake and subsided them into 8 proximate determinants grouped in three broad categories to facilitate quantification (Bongaarts 1978, Lucas 1994). Table 2.2 shows the complete 8 proximate determinants of fertility as developed by Bongaarts based on Davis and Blake’s ideas. Further, Bongaarts (1978) identified too that the majority of fertility variation is affected most by four key proximate causes which consist of:
Rising age at marriage reported in developing countries (National Research Council 2005) did not show meaningful increase in Nigeria. Median age at first marriage in Nigeria was 17.1 in 1990, 18.3 in 1999 and 17.2 in 2003 (NDHS
1990, 1999, 2003). The proportion of women that first married at exactly 15 years in Nigeria was twenty-eight percent, 24.3 percent and thirty percent in 1990, 1999 and 2003 respectively. The proportion of women married defined by Bongaarts as the proportion of childbearing women who are sexually active in their reproductive age and living in the stable sexual unions (marriage) (Bongaarts, 1978). Increase in the median age at marriage would favour decreased fertility and vice-versa. It was reported that the decline in median age at marriage increased fertility in Colombia, the Dominican Republic and Turkey (Bongaarts 2005). Early marriage increases the number of reproductive years in marriage with the concomitant exposure to risk of conception. High fertility as a result of early marriage was observed in Peru (Bongaarts 2005).
In Nigeria, contraceptive use has not yet contributed significantly to fertility decline at national level. The impact has been felt in urban areas and among women with higher education (Feyisetan and Bankole, 2002). Contraceptive usage had no effect on fertility in the northeast and limited effect by other background variables (NFS 1981/82). Marital disruption and contraception play reducing roles in urban fertility; this is though inadequate to offset the
factors supporting fertility increase in remote rural areas of Nigeria (Chimere, 1990b).
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1075
ISSN 2229-5518
Effects of contraception on fertility are weak in Nigeria and Cameroon whereas they are strong in the Ivory Coast and Ghana (Chimere, 1993). The differences in the contraceptive depressing magnitude may reflect changes in the contraceptive prevalence rate (CPR) and level of efficient use of contraception. However, there is an increasing trend in contraceptive use in Nigeria, especially the modern methods of contraception. Evidence from the WFS of
1981/82 shows that 6.2% of women that were exposed to the risk of childbearing were on contraception, out of
which 0.7% were effectively on the modern method (Feyisetan and Bankole, 2002). In 1990, 7.5% and 6% of all women and currently married women respectively were using contraception (Feyisetan and Bankole, 2002). Of the women were using modern methods of contraception (Feyisetan and Bankole, 2002). By 1999, the use of contraceptives had increased to sixteen percent for all women and about 9%. Currently, married women were at least
1.9 times more likely to use contraceptives in 1999 compared to 1990 (Oladosu, 2001). The use of contraception has been observed to be higher in the southern part of Nigeria especially the southwest, in urban areas and among highly educated women (NDHS final report 1999). It was also observed that the use of contraceptives in the rural areas has increased tremendously by 23 percent between 1990 and 1999 (Feyisetan and Bankole, 2002).
According to the DHS standard, there are three categories of contraceptive methods. They are as follows:
i) The modern methods: Female and male sterilization, female and male condoms, the pill, the intrauterine device (IUD), injectables, implants, diaphragm, foam or jelly.
ii) Traditional methods: Periodic abstinence (safe period or rhythm method) and withdrawal and, the lactational amenorrhoea (LAM).
iii) Other methods: Herbs, teas, grasses or other methods mentioned by the respondent.
Bongaarts (1978) found that lactations has an inhibitory effect on ovulation and thus increases the birth interval and reduces natural fertility by comparing average birth interval lengths in the presence and absence of lactation (Bongaarts, 1978). In Nigeria, contraceptive use has not yet contributed significantly to fertility decline at national level. The impact has been felt in urban areas and among women with higher education (Feyisetan and Bankole,
2002). Contraceptive usage had no effect on fertility in the northeast and limited effect by other background
variables (NFS 1981/82). Marital disruption and contraception play reducing roles in urban fertility, this is though inadequate to offset the factors supporting fertility increase in remote rural areas of Nigeria (Chimere, 1990b). Effects of contraception on fertility are weak in Nigeria and Cameroon whereas they are strong in the Ivory Coast and Ghana (Chimere, 1993).
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1076
ISSN 2229-5518
Induced abortion is defined by Bongaarts (1978) as any practice that deliberately interrupts the normal course of gestation (Bongaarts, 1978). By calculating the index (Ca ) which refers to the proportion by which fertility is reduced as the consequences of the practice of induced abortion, he found that Ca declines with increasing incidence of induced abortion (Bongaarts, 1978).
Others are Polygamy- having more than one wife at the same time, have implications for the frequency of sexual intercourse, and thus, may have an effect on fertility. Recent sexual activity, age at first marriage, age at first sexual intercourse and menopause.
Table 2.3 shows those seven proximate determinants given approximated rating for the two criteria based on other studies on the relationship between them and fertility.
Source: (Bongaarts, 1982)
Contextual determinants are those factors that affect fertility indirectly as they can only have effect on fertility through the proximate determinants (Bongaarts 1982; Lucas and Meyer 1994). As noted earlier, substantial insights
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1077
ISSN 2229-5518
can be gained if a study on fertility variance, levels, and trends is done by comprising analyses both on the proximate determinants and the contextual factors.
In Freedman’s view, reproductive decision is never left solely in the hands of individual couples because the control of fertility behaviour is so important to the society. In another words, the issue of how many children a couple should have is influenced by the ideal family size norms that apply to their society. Later Freedman (1975) proposed a framework for the sociological analysis of fertility levels. He discusses how the environment, mortality, social and economic structure (including the family planning program) develop the social norms about family size and the proximate determinants or intermediate fertility variables and hence control fertility (Freedman, 1975). Figure 2.3 summarizes those normative values in a society and their effects on fertility.
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1078
ISSN 2229-5518
Bongaarts (1978) proposed a simple but ingenious method of quantifying the relative effects of the proximate determinants of fertility in a given population. The model is based on the view that each of the proximate determinants of fertility- marriage/percent in union, breastfeeding and postpartum abstinence, contraception and induced abortion- is to reduce fertility in a given population.
This hypothetical level they referred to as the Total Fecundity rate (TF). The fertility actually observed in a given population reflects the extent to which the proximate determinants actually cause fertility in that fertility to diverge from the TF. Suppose that the observed fertility is measured by the period TFR. Bongaarts and Potter (1983) define two further measures: total marital fertility rate (TMFR) and total natural marital fertility rate (TN).
The difference between the TF and TN is accounted for by the prevalence of breastfeeding and postpartum abstinence in a population. Bongaarts and Potter refer to their joint efforts as postpartum infecundability. The difference between the TN and TMFR is accounted for by the prevalence of contraception induced abortion. Finally the difference between the TMFR and TFR measures the fertility-inhibiting effect of delayed marriage, non- marriage and marital disruption.
The model propose that four indices be calculated which quantify these fertility-inhibiting effects. They are defined as follows:
• Cm is an index of marriage, ranging in value from 1 if all women of reproductive age are married, to 0 in the absence of marriage;
• Cc is an index of contraception, ranging in value from 1 if no contraception is used in the population to 0 if all women use perfectly effective contraception;
• Ca is a index of induced abortion, ranging in value from 1 if abortion does not occur to 0 if all pregnancies are aborted;
• Ci is an index of postpartum infecundability, ranging in value from 1 if there is no breastfeeding or postpartum abstinence, to 0 in the (rather improbable) case that the duration of infecundability is infinite.
Total fecundity rate (TF)
Total natural marital fertility rate (TN)
Total marital fertility rate (TMFR)
Total fertility rate (TFR)
Ci
Cc * Ca
13 Cm
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1079
ISSN 2229-5518
The relationship between these four indices and the four fertility rates listed above is as follows: Cm = TFR/TMFR (1)
Cc x Ca = TMFR/TN (2) Ci = TN/ TF (3)
Substituting equation (3) into equation (2) and then into equation (1) produces equation (4) TFR = Cm x Cc x Ca x Ci x TF (4)
This last equation (4) simply summarizes the relationship between the TFR and the four most important proximate determinants.
In a later paper, Bongaarts added a fifth proximate determinant, the pathological sterility (Bongaarts et al. 1984). The fertility-inhibiting effect of pathological sterility is measured in the model by the index of pathological sterility (Bongaarts et al. 1984). The presence of the fifth proximate determinant changes the original model. As a result, the new complete model estimate of TFR is:
TFR = Cm x Cc x Ca x Cs x Ci x TF
where
Cm = index of marriage or proportion married
Ci = index of post partum infecundibility
Ca = index of abortion
Cs = index of sterility
Cc = index of contraception
TF = total fecundity
PPI = duration of post partum infecundibility (in months) TAR = Total Abortion Rate
Sterility = Percentage of women aged 45-49 who are childless
Prevalence = Percentage of women of reproductive age using contraception
Effectiveness = Average effectiveness of contraception
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1080
ISSN 2229-5518
The analysis was carried out using the Bongaarts model which was facilitated by the ProxDemo software (The
Future Groups 1997). The basic model is: TFR = Cm x Ci x Ca x Cs x Cc x TF
The formulae are as stated below;
Cm = percentage of women of reproductive age in union
Ci = 20 / (18.5 + PPI)
Ca = TFR / (TFR + 0.4 × (1 - Prevalence) × TAR) Cs = (7.63 - 0.11 × Sterility) / 7.3
Cc = 1 - 1.08 × (Prevalence) × (Effectiveness)
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1081
ISSN 2229-5518
The study estimated the fertility reduction contribution of the proximate determinants by using the proximate determinants analysis software called Proxdemo (The Futures Group, 1997). Input data needed for the analyses - proportion of currently married women, percentage distribution of contraception methods currently used, median duration of breastfeeding, mean duration of postpartum infecundability, and the TFRs were taken from the final reports of the 2003 and 2008 NDHS surveys. The results of analysis on the proximate determinants of fertility for the 2003 and 2008 NDHS surveys are shown in Table 4.1 and 4.2 respectively. Also, the complete output of the analysis done using proxdemo software are shown in appendix I and appendix II for NDHS 2003 and 2008 respectively.
Table 4.1a The Effects of Proximate Determinants on Fertility, Nigeria. 2003 NDHS using Bongaarts model
Proximate Determinants | Individual Effect | Percentage Contribution to Reduction |
Total fecundity Percent in union Post partum infecundability Sterility Contraception Total Fertility Rate (TFR) | 12.61 -4.04 -3.01 0.23 -0.10 5.70 | 100.0 30.7 23.0 1.7 0.8 43.8 |
Table 4.1b The Effects of Proximate Determinants on Fertility, Nigeria. 2008 NDHS using
Bongaarts model
Proximate Determinants Individual Effect Percentage Contributions to
Reduction
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1082
ISSN 2229-5518

The result captured that percent in union gave the highest contribution in reduction of fertility level in Nigeria for about 30.7%, followed by other proximate determinants; postpartum infecundability (23%), sterility (1.7%) and contraception (0.8%).
The result captured that percent in union gave the highest contribution in reduction of fertility level in Nigeria for about 30.8%, followed by other proximate determinants; postpartum infecundability (23.5%), sterility (1.7%) and contraception (0.8%).
The relationship between the proximate determinants and fertility had been analysed using Bongaarts model which was facilitated by the ProxDemo software (the results of which are discussed in section 4.3). Thus, this section aimed at describing the relationship between contextual determinants and proximate determinants of fertility. Bi- variate analysis was conducted only for the 2008 NDHS data assuming that this could produce the most recent illustration of the relationship between the contextual determinants and the proximate determinants of fertility.
No. | Contextual Determinant | Category | p value |
1. | Current age | 15-24 25-34 35-49 | 0.00 |
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1083
ISSN 2229-5518
2. | Educational level | No education Primary Secondary or higher | 0.00 |
3. | Wealth quintile | Low Middle High | 0.00 |
4. | Zones | North Central North East North West South East South South South West | 0.00 |
5 | Type of Residence | Rural Urban | 0.00 |
Dependent variable: (1) Currently Using (2) Not Currently Using
No. | Contextual Determinant | Category | p value |
1. | Current age | 15-24 25-34 35-49 | 0.00 |
2. | Educational level | No education Primary Secondary or higher | 0.00 |
3. | Wealth quintile | Low Middle High | 0.00 |
4. | Zones | North Central North East North West | 0.00 |
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1084
ISSN 2229-5518
South East South South South West | |||
5. | Type of Residence | Rural Urban | 0.00 |
Dependent variable: no co-wives (1) and one or more co-wives (2).
We reject H0t (t = 1, 2, 3, 4, 5) since their p-values are < 0.05 and conclude that current age, educational level, wealth quintile, zones and type of residence have a significant effect on current use of contraceptive use.
We reject H0t (t = 6, 7, 8, 9, 10) since their p-values are < 0.05 and conclude that current age, educational level, wealth quintile, zones and type of residence have a significant effect on polygyny.
The aim of this study was channeled at identifying the fertility reduction contribution of the proximate determinants of fertility among currently married women in Nigeria. As described in the literature reviewed, the fertility level in a population is influenced by several factors which are recognized as proximate and contextual determinants of fertility. Based on the assumption explained on this study’s theoretical framework, fertility behavior is linked to its proximate (direct) and contextual (indirect) determinants. The direct or proximate ones (consist of current use of contraception, polygamy, age at first marriage and duration of breastfeeding) affect fertility directly. Meanwhile, the contextual factors could influence fertility level only through proximate determinants. To achieve this objective, analyses were carried out on the effects of the proximate determinants on fertility and on differences in trends in the proximate determinants during the period of 2003-2008. These determinants could affect fertility directly or indirectly. Hence, the various methods of analyses used different techniques to examine the objectives. Firstly, the study used ProxDemo software to identify the contribution of each proximate determinant (age at first marriage,
contraceptive use, and duration of breastfeeding), in reducing the fertility level. Then, it used the Chi‐Square test to
examine the relationship between some of the independent (contextual determinants) and the dependent (proximate
determinants) variables.
An analysis of the contribution of each proximate determinant on the fertility level has found that percent in union has the greatest effect on fertility reduction compared to other proximate determinants. This is different from the
result gotten by Ibisomi (2008), where she arrived at the conclusion that post-partum in fecundability had the
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1085
ISSN 2229-5518
greatest inhibiting effect on fertility; followed by marriage/sexual activity, contraception and then sterility. It revealed that percentage of women in union which is same as proportion of married women contributed 30.8 % to fertility reduction in Nigeria. Meanwhile, it showed that the effect on the reduction of contraceptive prevalence 0.8% in this province was lower compared to the proportion of married women and post partum infecundability. Indeed, Bongaarts (1982) stated that it was one of the proximate determinants with the highest effect on the fertility level (Bongaarts 1982). The analyses of the proximate determinants also shows variations in Nigerian total fertility over time as seen section 4.2, it revealed that in general there were virtually no changes observed in all proximate determinants, namely postpartum infecundability contraception, sterility and percentage in union, between the two successive surveys.
Analysis of differences in trends in proximate determinants of fertility between the 2003 and the 2008 NDHS were conducted in age at first marriage, current use of contraception, and duration of breastfeeding as shown in section
4.3. Overall, there had been a substantial change in age at first marriage as it rose from 16.6 years to 18.3 years. This suggests that Nigerian women have married at a later age over time. Generally, the trend towards increasing age at first marriage occurred across women from different background characteristics, most notably by age, residence,
zones and education, which all led to a negligible reduction in fertility rate.
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1086
ISSN 2229-5518
Analyses of the effects of proximate determinants on fertility showed that there had been virtually no changes observed during the period of 2003-2008, although percent in union remained the most important proximate determinant in contributing to fertility reduction in Nigeria.
Analyses of trends in the proximate determinants of fertility indicated that both overall and across, women of different backgrounds age at first marriage rose from 16.6years to 18.3years. In general, contraceptive use increased from 12.6% to 14.6%. Duration of any type of breastfeeding – any breastfeeding, exclusive breastfeeding, or predominantly breastfeeding – had declined among both male and female children, and women of different residence, educational attainment, zones and wealth quintile.
Analyses on the relationship between contextual determinants and the proximate determinants of fertility suggested that each of the contextual determinants i.e. current age in 5-year groups, wealth quintile, zones, educational level, and type of place of residence had a statistically significant relationship with each of the proximate determinants i.e. current use of contraception, and polygamy.
The use of contraception is still very low in Nigeria and this is a major factor that contributes to the reduction of fertility, the policy makers should organize awareness programmes both for the educated and the non-educated women in Nigeria to encourage the use of contraception which in turn would contribute to fertility reduction.
The health care policy makers should encourage the practice of breastfeeding for at least 6 months as this would extend postpartum amenorrhea and in turn postpartum infecundability and birth intervals to ensure continued decline in fertility.
In regard to the proximate determinants of fertility, this study could not cover induced abortion due to the unavailability of information, the National population Commission Agency should put this into
consideration by the next Nigeria Demographic Health and Survey to reduce error in the data collected.
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013 1087
ISSN 2229-5518
Andy Field, (2005). Discovering Statistics Using SPSS, Second Edition, pp. 688-697.
Bongaarts, J 1978, “A Framework for Analyzing the Proximate Determinants of Fertility”,Population and Development Review, Vol. 4, No. 1, March, pp. 105-132, retrieved 08June 2012, http://www.jstor.org.ezproxy.flinders.edu.au/stable/pdfplus/1972149.pdf.
Bongaarts, John, (1982), The fertility‐inhibiting effects of the intermediate fertility variables,Studied in Family Planning, Vol.13, No.6/7,
pp. 189.
Bongaarts, J. & Potter, R. (1983). Fertility, biology, and behavior: an analysis of theproximate determinants. New York Academic Press. Bongaarts, J. & Lesthaeghe, R. (1984). The Proximate Determinants of Fertility in Sub Saharan Africa. Population and Development Review.
511-537.
Bongaarts, J. (2008). Fertility transition in developing countries: progress or stagnation. Studies in Family Planning, 39 (2), 105-110. Caldwell, J. et al. (1992). Fertility decline in Africa: A new type of transition? Population and Development Review.
Chimere, O. (1990a). Proximate determinants of fertility in Nigeria. Journal of Social biology Fall-Winter; 37 (3-4), 162-71.
Chimere, O. (1990b). Determinants of rural and urban fertility differentials in Nigeria. Journal of Biosocial Science, 22, 293-303.
Davis, Kingsley & Blake, Judith, (1956). Social structure and fertility: an analytical framework’, Economic Development and Cultural Change, Vol.4, No.2, pp. 211-235
Feyisetan, B. & Togunde, O. (1988). Indices of women’s status and fertility in Nigeria. Genus XLIV, Nos. 1-2, pp. 229-247.
Feyisetan B.J. & Bankole, A. (2002). Fertility transition in Nigeria: Trends and prospects, http://www.Un.org/esa/population/Publications/completingfertility/Revised BANKOLEpaper.PDF.
Freedman, R 1997, “Do Family Planning Programs Affect Fertility Preferences? A Literature Review,” Studies in Family Planning, Vol.
28, No. 1, March, pp. 1-13, http://www.jstor.org.ezproxy.flinders.edu.au/stable/pdfplus/2137966.pdf.
Guttmacher, (2008). Fertility declines have stalled in many countries in Sub-Saharan Africa.Family planning perspectives.
Harwood-Lejeune, A. (2001). Rising age at marriage and fertility in Southern and Eastern Africa. European Journal of Population 17 (3), 261-
280.
Isiugo-abanihe, U. C. (1997). Fertility preferences and contraceptive practice in Nigeria. Annals of Social Sciences Council of Nigeria, 9, 1-20. Kiersten Johnson et al (2011). Changes in the Direct and Indirect Determinants of Fertility in Sub-Saharan Africa. DHS Analytical Studies No.
23. Calverton, Maryland, USA: ICF Macro.
Kranzler, G and Moursund, J 1999, Statistics for the Terrified, 2nd edn, Prentice-Hall, NewJersey.
Lucas, D 1994, “The Proximate Determinants of Fertility,” in Beginning Population Studies, D Lucas and P Meyer (eds), 2nd Ed., National Centre for Development Studies, The Australian National University, Canberra, pp. 44-55.
IJSER © 2013 http://www.ijser.org
International Journal of Scientific & Engineering Research, Volume 4, Issue 11, November-2013
ISSN 2229-5518
1088
Makinwa-Adebusoye, P. K. & Feyisetan, B. J. (1994). The quantum and tempo of fertility in Nigeria. In Macro International Inc. Fertility Trends and Determinants in Six African Countries, DHS Regional Analysis Workshop for Anglophone Africa, 41-86
McNicol!, G & Singarimbun, Masri, 1982, Fertility Decline in Indonesia: Background and Proximate Determinants.