Of cross-sectional views of the patient are taken using magnetic-resonance-imaging or x-ray methods. This kind of imaging is necessary for all types of operative procedure and, as such, does not differ from traditional surgical techniques.
International Journal of Scientific & Engineering Research Volume 2, Issue 8, Auguest-2011 1
ISSN 2229-5518
Applications of Robotics in Medicine
Paduri Veerabhadram
Abstract- Robots in medicine deserve enhanced attention, being a field where their instrumental ids enable exacting options. The availability of oriented effectors, capable to get into the human body with no or negligible impact, is challenge, evolving while micro-mechanics aims at nanotechnology. The survey addresses sets of known achievements, singling out noteworthy autonomous in body devices, either co-robotic surgical aids, in view of recognizing shared benefits or hindrances, to explore how to conceive effective tools, tailored to answer given demands, while remaining within established technologies. Robotics for medical applications started fifteen years ago while for biological applications it is rather new (about five years old). Robotic surgery can accomplish what doctors cannot because of precision and repeatability of robotic systems. Besides, robots are able to operate in a contained space inside the human body. All these make robots especially suitable for non- invasive or minimally invasive surgery and for better outcomes of surgery. Today, robots have been demonstrated or routinely used for heart, brain, and spinal cord, throat, and knee surgeries at many hospitals in the United States (International Journal of Emerging Medical Technologies, 2005). Nanorobotics is the still largely hypothetical technology of creating machines or robots at or close to the scale of a nanometer(10-9meters). Also known as nanobots or nanites, they would be constructed from nanoscale or molecular components. So far, researchers have only been able to produce some parts of such a machine, such as bearings, sensors, and synthetic molecular motors, but they hope to be able to create entire robots as small as viruses or bacteria, which could perform tasks on a tiny scale. Possible applications include micro surgery (on the level of individual cells), utility fog, manufacturing, weaponry and cleaning. This presentation provides a survey of current developments, in the spirit of focusing the trends toward the said turn.
—————————— ——————————
R obotics is a field that has many exciting potential applications. It is also a field in which expectations of the public often do not match current realities. Truly incredible capabilities are being sought and demonstrated in research laboratories around the world. However, it is very difficult to build a
The word robot (from the Czech word robota meaning compulsory labor) was defined by the Robotic Institute of America as “a machine in the form of a human being that performs the mechanical functions of a human being but lacks sensitivity.” One of the first robots developed was by Leonardo da Vinci in 1495; a mechanical armored knight that was used to amuse royalty. This was then followed by creation of the first operational robot by Joseph Marie Jacquard in 1801, in which an automated loom, controlled by punch cards, created a reproducible pattern woven into cloth. Issac Asimov further elucidated the role of robotics in 1940 through short stories; however, it was his three laws of robotics that received popular acclaim. The three laws state1) A robot may not injure a human being, or through inaction allow a human being to come to harm2)A robot must obey the orders given it by human beings except where such orders would conflict with First Law and 3) A robot must protect its own existence as long as such protection does not conflict with the First or Second Law
mechanical device (e.g., a robotic arm) that has dexterity comparable to a human‟s limbs. It is even more difficult to build a computer system that can perceive its environment, reason about the environment and the task at hand, and control a robotic arm with anything remotely approaching the capabilities of a human being.
Robots are filling an increasingly important role of enhancing patient safety in the hurried pace of clinics and hospitals where attention to details and where reliability are essential. In recent years, robots are moving closer to patient care, compared with their previous role as providing services in the infrastructure of medicine. Examples of past use are in repetitive activities of cleaning floors and washing equipment and carrying hot meals to patients‟ bedside. What is new is finding them in clinical laboratories identifying and measuring blood and other specimen for testing, and in pharmacies counting pills and delivering them to nurses on „med-surg-units‟ or ICU‟s. Or bringing banked blood from the laboratory to the ED, surgery, or ICU for transfusions. Robots are being used as very accurate
„go-fors‟!
An early active robot, „Robodoc‟ was designed to mill perfectly round lumens in the shafts of fractured bones, to improve the bonding of metal replacements such as for femur heads, and knee joints. The future of this system remains uncertain because of questions about the ultimate beneficial outcomes.
The reasons behind the interest in the adoption of medical robots are multitudinous. Robots provide
IJSER © 2011
International Journal of Scientific & Engineering Research Volume 2, Issue 8, Auguest-2011 2
ISSN 2229-5518
industry with something that is, to them, more valuable than even the most dedicated and hard-working employee – namely speed, accuracy, repeatability, reliability, and cost-efficiency. A robotic aid, for example, one that holds a viewing instrument for a surgeon, will not become fatigued, for however long it is used. It will position the instrument accurately with no tremor, and it will be able to perform just as well on the 100th occasion as it did on the first.
Robotic surgery is the process whereby a robot actually carries out a surgical procedure under the control of nothing other than its computer program. Although a surgeon almost certainly will be involved in the planning of the procedure to be performed and will also observe the implementation of that plan, the execution of the plan will not be accomplished by them - but by the robot.
In order to look at the different issues involved in the robotic fulfillment of an operation, the separate sections of a typical robotic surgery (although robotic surgery is far from typical) are explained below.
Surgical planning consists of three main parts. These are imaging the patient, creating a satisfactory three- dimensional (3D) model of the imaging data, and planning/rehearsing the operation. The imaging of the patient may be accomplished via various means. The main method is that of computer tomography (CT). CT is the process whereby a stack
Of cross-sectional views of the patient are taken using magnetic-resonance-imaging or x-ray methods. This kind of imaging is necessary for all types of operative procedure and, as such, does not differ from traditional surgical techniques.
A patient having a brain scan
This two-dimensional (2D) data must then be converted into a 3D model of the patient (or, more usually, of the area of interest). The reasons for this transformation are twofold. Firstly, the 2D data, by its very nature, is lacking in information. The patient is, obviously, a 3D object and, as such, occupies a spatial volume. Secondly, it is more accurate and intuitive for a surgeon, when planning a procedure, to view the data in the form that it actually exists. It should be noted, however, that the speed of said hardware is increasing all the time and the price will decrease too, as the technology involved becomes more commonplace. This means that the process will be more cost-efficient and increasingly routine in the future.
The third phase of the planning is the actual development of the plan itself. This involves determining the movements and forces of the robot in a process called „path planning‟ - literally planning the paths that the robot will follow.
It is here that the 3D patient model comes into play, as it is where all the measurements and paths are taken from. This emphasizes the importance of the accuracy of the model, as any errors will be interpreted as absolute fact by the surgeons (and hence the robot) in their determination of the plan.
The registration of the robot and the patient is the correlation of the robot‟s data about the patient with the actual patient, in terms of positioning. There are two important stages in the registration procedure - fixation of the patient and the robot, and intra-surgical registration itself. Fixation is an essential ingredient of a successful robotic operation. Robots act upon pre- programmed paths , these programs are much more complex if they must take into account the fact that the patient‟s position may be different to the inputted data and, in fact, continually changing. For this reason it is imperative that the robot can act in, at least, a semi- ordered environment.
IJSER © 2011
International Journal of Scientific & Engineering Research Volume 2, Issue 8, Auguest-2011 3
ISSN 2229-5518

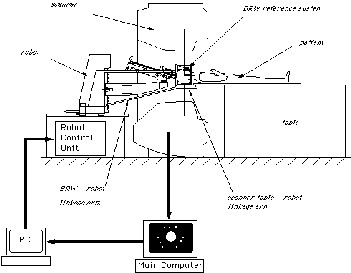
Fixation of the patient that is fixing the patient in position (i.e. on the operating table), is achieved through strapping and clamping of the areas pertinent to the surgery. This is common in traditional surgery, too. For example, the head is fixed in position during neurosurgery through the application of a head-fixation device known as a „stereo tactic unit‟. Fixation of the robot is achieved through analogous methods.
The intra-surgical registration itself is the process of establishing a common reference frame between the pre-surgical data (3D model and associated surgical plan) and the corresponding patient anatomy. There are two primary techniques of achieving this common frame of reference.
The first, and most usual, method is to attach fiducial to the underlying patient structures pre- operatively. These fiducial are then sensed, and compared to the pre- operative data, to precisely align the two data sets. Furthermore, these fiducial are invasive and cause added trauma to the patient in sites physically far from the primary field of surgical focus. The alternative to fiducially-based registration is that of „surface- based‟ registration. This technique uses surfaces that are intrinsic to the data itself. The benefit of this method is that it does not require the use of expensive and traumatically invasive markers.The illustration of the implementation of this concept is shown below. On the Left (a) is a brain with extracted curves shown in red. On the right (b) is the final 3D model gained from these curves:
The success of surface-registration is highly dependent upon the realism and accuracy of the 3D models gained pre-operatively and upon the sensing accuracy of intra- surgical data acquisition. Geometric surface model validation is complicated since errors can be introduced at several stages of model creation: during imaging,
„segmentation‟ and surface creation. Prior to the emergence of surface-based techniques for surgery, 3D modeling medical data has been primarily used as a teaching aid in the study of anatomy (e.g. VOXEL- MAN). These models have very different accuracy requirements to those used for surface-based registration.
Once all of the preparation is complete, it is time to pass control to the robot for the actual implementation of the surgery. The robots used for automated surgery tend, at the present time, to be adapted industrial robots; for example, the PUMA robot arm. Having brought up the fact that the surgeon is reliant upon the engineering behind the tools that
they are using, it is clear that companies would not wish to risk possible legal proceedings should one of their products fail. Once the robotic procedure is initiated, sensors collect real-time data from the operating site and pass this to a display, via which the surgeon observes the operation.
IJSER © 2011
International Journal of Scientific & Engineering Research Volume 2, Issue 8, Auguest-2011 4
ISSN 2229-5518
While, in robotic surgery, the robot is given some initial data information and allowed to proceed on its own, there are some other applications of robotics in surgery where the robot is actually guided by a human throughout the process. The actions of the robot are not predetermined, but rather controlled in real-time by the surgeon. The remote location can be as far away as the other side of the world, or as near as the next room. Since there is distance separating the surgeon and the patient, it is evident that the surgeon cannot operate using his own hands. A robot, local to the patient, becomes the surgeon‟s hands, while an intricate interface conveys the robot‟s senses to the surgeon (making use of while an intricate interface conveys the robot‟s senses to the surgeon (making use of visual, aural, force and tactile feedback).
In the sense that the robot is the one performing the surgery, telesurgery is a part of robotic surgery. Furthermore, as in robotic surgery, the patient is usually imaged before the operation starts and the information sent to the surgeon. In telesurgery the surgeon cannot rely on anything but the sensor data, which is transmitted from the remote location. The sensor data, therefore, must be absolutely correct. For this purpose, a host of different schemes are used
Telesurgery is mainly used as a form of minimally
invasive surgery. In traditional surgery, the physical
hand size has always been a limiting factor when it
comes to delicate surgery in hard-to-reach places. Since
the robot can theoretically be as small as is desired, it
can enter through a small opening, navigate through the body and finally reach and operate in places that would
otherwise be inaccessible without a large incision made specifically to facilitate entry. Recent experiments even involve the robot being inserted through a small puncture in the thigh and guided all the way to the brain through blood vessels as narrow as 1.5mm in diameter.
Robots in future
A nanometre is just one-millionth of a millimetre in length and nanotechnology involves studying and working with materials on an ultra-small scale. Using nanotechnology, scientists have created a tiny walking nanobot, using only the building blocks of life: DNA. The microscopic walker, which is only 10 nanometres long, uses its legs to move along a footpath. Nanotechnology could also lead to a range of materials with new qualities such as stay-clean glass and magnetic liquids. There may also be breakthroughs from scientists trying to implant computer programs into living creatures - known as wetware. This technology could help people with false arms or legs to move them just by thinking about it.
IJSER © 2011
International Journal of Scientific & Engineering Research Volume 2, Issue 8, Auguest-2011 5
ISSN 2229-5518

"Safety Critical Problems In Medical Systems", Brian Davies, Proceedings of
the Second Safety-Critical Systems Symposium, pp. 55-68
[4] "An experimental telesurgery robot", G.C. Thorne, M. Halliwell, P.N.T. Wells,
IEE Colloquium on 'Towards Telesurgery', No. 1995/137, pp. 4/1-4 “The Karlsruhe Endoscopic Surgery Trainer", Forschungszentrum Karlsruhe
Technik und Umwelt.
[5] “Telepresence surgery", SRI Center for Medical Technology
“Medical Robotics", Lara Crawford, Robotics Lab, University of
Berkeley, California
Medical robotics, and particularly autonomous surgical robotics, is still in an embryonic stage. To conclude, there are several steps that must be taken in order to further the use and development of robots in surgery (and in medicine in general). These are:
The development, and international adoption, of safety standards the aim of task-specific, as opposed to general-purpose, robots the education of the medical community in the acceptance and integration of Robots . The economic and social advantages to be gained from the mass-use of robotics in medicine (and particularly surgery), as already expounded, are enormous. If all of the above steps are taken, then the full potential of robotics can be exploited in the medical sector, as it has been in industrial applications, for the improved welfare of society everywhere.
[1]"Robotics in Medicine", P.Dario, E.Guglielmelli, B.Allotta, IROS
'94.
Proceedings of the IEEE/RSJ/GI International Conference on
Intelligent Robots
and Systems. Advanced Robotic Systems and the Real World
(Cat.No.94CH3447-0), Sept.1994, Vol.2, pp.739-52
[2] "A Robot with Improved Absolute Positioning Accuracy for
CT Guided
Stereotactic Brain Surgery", Y.S.Kwoh, J.Hou, E.A. Jonckheere, S.Hayati , IEEE
Transactions on Biomedical Engineering, Vol.35, Feb.1988, pp.153-60
"3D image reconstruction and its application to surgery automation",
[3]C.H.Cheng, W.H.Yeng, M.C.Tsai, H.B.Hsieh, Proceedings of the Third
International Conference on Systems Integration, Aug.1994, pp.967-73
IJSER © 2011